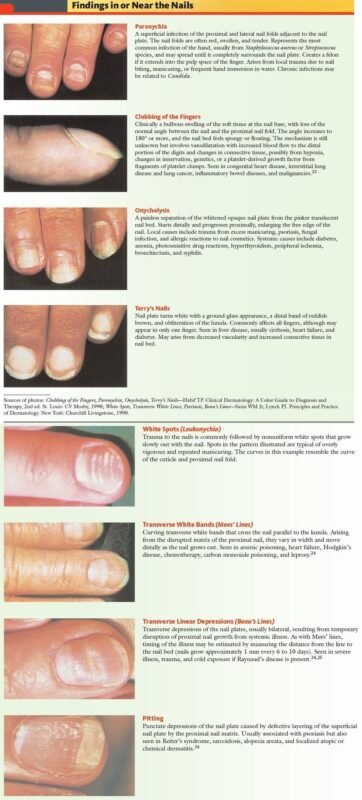
What Is Paronychia?/Paronychia is an infection of the proximal and lateral fingernails and toenails folds, including the tissue that borders the root and sides of the nail. This condition can occur spontaneously or following trauma or manipulation. Paronychia is among the most common infections of the hand. Paronychia results from the disruption of the protective barrier between the nail and the nail fold, introducing bacteria and predisposing the area to infection. Acute paronychia is usually limited to one nail; however, if drug-induced, it can involve many nails.[rx][rx]
Paronychia is an inflammatory process of the nail fold. Acute paronychia is most often the result of bacterial infection, commonly from Staphylococcus aureus. Chronic paronychia is usually caused by Candida albicans. The predisposing factor in the production of chronic paronychia is trauma or maceration producing a break in the seal (cuticle) between the nail fold and the nail plate. This break produces a pocket that holds moisture and promotes the growth of microorganisms.

Types of Paronychia
The classification of paronychia is according to the clinical presentation:
-
Acute paronychia – lasting less than six weeks, painful and purulent condition; most frequently caused by a bacterial infection, especially staphylococci.
-
Chronic paronychia – usually caused by mechanical or chemical factors and sometimes infectious etiology like a fungal infection, especially Candida species. Risk factors include occupation (dishwasher, bartender, housekeeper), certain medications, and immunosuppression (diabetes, HIV, malignancy).
- Prosector’s paronychia – is a primary inoculation of tuberculosis of the skin and nails, named after its association with prosectors, who prepare specimens for dissection. Paronychia around the entire nail is sometimes referred to as runaround paronychia.
- Painful paronychia – in association with a scaly, erythematous, keratotic rash (papules and plaques) of the ears, nose, fingers, and toes may be indicative of acrokeratosis paraneoplastic, which is associated with squamous cell carcinoma of the larynx.
Classification can also be by etiology
-
Bacterial, commonly staphylococci
-
Viral, commonly Herpes simplex virus
-
Fungal, commonly Candida species
Noninfectious causes of paronychia can include contact irritants, excessive moisture, and medication reaction.[rx]
Alternatively, paronychia may be divided as follows
- Candidal paronychia – is an inflammation of the nail fold produced by Candida albicans.[rx]
- Pyogenic paronychia – is an inflammation of the folds of skin surrounding the nail caused by bacteria.[rx] Generally, acute paronychia is a pyogenic paronychia as it is usually caused by a bacterial infection.[rx]
According to diagnostic Criteria of paronychia are
- Cellulitis – Cellulitis is a superficial infection and will present as erythema and swelling to the affected portion of the body with no area of fluctuance. Treatment is with oral antibiotics.
- Felon – A felon is a subcutaneous injection of the digital pulp space. The area becomes warm, red, tense, and very painful due to the confinement of the infection, creating pressure in the individual compartments created by the septa of the finger pad. These require excision and drainage, usually with a longitudinal incision and blunt dissection to ensure adequate drainage.
- Herpetic whitlow – This is a viral infection of the distal finger caused by HSV. Patients usually develop a burning, pruritic sensation before the infection erupts. A physical exam will show vesicles, vesicopustules, along with pain and erythema. It is important to not confuse this with a felon or a paronychia as incision and drainage of herpetic whitlow could result in a secondary bacterial infection and failure to heal.
- Onychomycosis – This is a fungal infection of the nail that causes whitish-yellowish discoloration. Sometimes difficult to treat and requires oral antibiotics instead of topical.
- Nail Psoriasis – psoriasis can also affect the fingernails and toenails. It may cause thickening of the nails with areas of pitting, ridges, irregular contour, and even raising of the nail from the nail bed.
- Squamous cell carcinoma – Squamous cell carcinoma is mainly cancer of the skin but can also affect the nail bed. It is a rare malignant subungual tumor subject to misdiagnosis as chronic paronychia.[rx][rx]

Causes of Paronychia
- Acute paronychia is usually due to bacterial infection with Staphylococcus aureus (which may be multiresistant), Streptococcus pyogenes, Pseudomonas, or other bacterial pathogens. It can also be due to the cold sore virus, Herpes simplex, and the yeast, Candida albicans.
- The cause or causes of chronic paronychia are not fully understood. In many cases, it is due to dermatitis of the nail fold. Often several different micro-organisms can be cultured, particularly Candida albicans and the Gram-negative bacilli, pseudomonas.
- Infections (Bacterial, mycobacterial, or viral)
- Raynaud’s disease
- Metastatic cancer, subungual melanoma, squamous cell carcinoma. Benign and malignant neoplasms should always be excluded when chronic paronychia does not respond to conventional treatment
- Papulosquamous disorders like psoriasis, vesiculobullous disorders-pemphigus
- Drug toxicity from medications such as retinoids, epidermal growth factor receptor inhibitors (cetuximab), and protease inhibitors. Indinavir- induces retinoid-like effects and remains the most frequent cause of chronic paronychia in patients with HIV disease.
- Retinoids also induce chronic paronychia. The mechanism can be -nail fragility and minor trauma by small nail fragments.[rx] Paronychia has also been reported in patients taking cetuximab (Erbitux), an anti-epidermal growth factor receptor (EGFR) antibody used in the treatment of solid tumors.[rx]
- Acute paronychia is usually caused by bacteria. Paronychia is often treated with antibiotics, either topical or oral or both. Chronic paronychia is most often caused by a yeast infection of the soft tissues around the nail but can also be traced to a bacterial infection. If the infection is continuous, the cause is often fungal and needs antifungal cream or paint to be treated.[rx]
- Repeatedly washing hands and trauma to the cuticle such as may occur from repeated nail-biting. In the context of bartending, it is known as bar rot.[rx]
Paronychia can occur with diabetes, drug-induced immunosuppression,[rx] or systemic diseases such as pemphigus.[rx]
Symptoms of Paronychia
- The skin typically presents as red, itchy, and hot, along with intense pain. Pus is usually present, along with gradual thickening and browning discoloration of the nail plate.
- Red, scaly, itchy or raised patches
- Patches may be redder on outside edges or resemble a ring
- Patches that begin to ooze or develop a blister
- Bald patches may develop when the scalp is affected
- Nails may thicken, discolor or begin to crack[rx]
- Cracking and peeling skin on your feet, most commonly between your toes and on your soles
- Dry skin on your soles or sides of your feet
- Raw skin on your feet
- Discolored, thick, and crumbly toenails
- Toenails that pull away from the nail bed
- Itchy erosions and/or scales between the toes, especially between 4th and 5th toes
- Scale covering the sole and sides of the feet (hyperkeratotic/moccasin type, usually caused by T. rubrum)
- mall to medium-sized blisters, usually affecting the inner aspect of the foot (vesiculobullous type).
- It can also uncommonly cause oozing and ulceration between the toes (ulcerative type), or pustules (these are more common in tinea pedis due to T. interdigitale than that due to T. rubrum).
Diagnosis of Paronychia
- Digital Pressure Test – Diagnostic for early Paronychia with abscess before abscess is clearly demarcated. The patient opposes the thumb and affected finger (applying pressure to a pulp on the volar aspect at fingertip). Abscess becomes demarcated with blanching
- CBC, ESR, Hb test – It is basically done for blood-related infection and others
- Urine Examination– It is done to investigate the infection of urine with other problems.
- RBS ( Random blood sugar)
- Serum creatinine – examination for the diagnosis of kidney problems.
Laboratory investigations
The following are the various laboratory tests that can be used for confirming a diagnosis of dermatophytosis.
- Direct microscopic examination – [rx] Treatment of skin specimen with 10–20% potassium hydroxide (KOH) is a quick and inexpensive bedside tool to provide evidence of dermatophyte infection. Fluorescent staining with optical brighteners (diamino stilbene) is the most sensitive method to microscopically detect fungi in skin scales as well as in specimens from nails and hair.[rx] These substances bind to chitin, the main cell wall component of fungi
- Culture and antifungal sensitivity – [rx] Sabouraud dextrose agar (SDA, 4% peptone, 1% glucose, agar, water) is the most commonly used isolation media for dermatophytosis and serves as the medium on which most morphologic descriptions are based. The development of the colony takes 7–14 days. Modified SDA, with the addition of gentamicin, chloramphenicol, and cycloheximide is more selective for dermatophytes as chloramphenicol inhibits the growth of saprophytic fungus. The dermatophyte test medium is an alternative to isolation media that contain pH indicator phenol red. It is incubated at room temperature for 5–14 days.
Antifungal Susceptibility Testing
- Microdilution method – The broth microdilution assay for antifungal susceptibility testing of dermatophytes has been previously developed as a modification of the Clinical and Laboratory Standards Institute M38-A2 standard method. The final concentrations of terbinafine and itraconazole used is 0.06–32.0 μg/ml and for fluconazole, 0.13–64.0 μg/ml.[rx] A standardized inoculum is prepared by counting the microconidia microscopically. Cultures are grown on SDA slants for 7 days at 35°C to produce conidia.
- Sterile normal saline (85%) – is added to the agar slant, and the cultures are gently swabbed with a cotton-tipped applicator to dislodge the conidia from the hyphal mat. The suspension is transferred to a sterile centrifuge tube, and the volume is adjusted to 5 ml with sterile normal saline. The resulting suspension is counted on a hemacytometer and is diluted in RPMI 1640 medium to the desired concentration.
- Minimum fungicidal concentration (MFC) determination – For determination of the MFC, 100-μl aliquots are removed from the assay wells showing no visible growth at the end of incubation and streaked onto SDA plates. The plates are incubated at 30°C for 7 days. The MFC is defined as the lowest drug concentration at which no visible fungal growth or colonies developed
- Dermatophyte identification – This can be based on colony characteristics, microscopic morphology, and physiologic tests. Dermatophytes can be distinguished based upon their morphology of the macroconidia. Few physiological tests are available which help in confirmation of certain species.
Histopathology
- Histology may be used in the diagnosis of Majocchi’s granuloma in which KOH examination of scale on the surface may more often be negative.
- When present, hyphae may be appreciated in stratum corneum on hematoxylin and eosin staining. Special stains most commonly used are periodic acid-Schiff and Gomori methenamine silver which helps to highlight hyphae.
Dermoscopy
- The comma hairs, which are slightly curved, fractured hair shafts, and corkscrew hair shave been described as the dermoscopic marker of tinea capitis. Broken and dystrophic hairs are also seen. However, in tinea corporis, the involvement of vellus hair as seen on dermoscopy is an indicator of systemic therapy.[rx]
Polymerase chain reaction and nucleic acid sequence-based amplification
These tests not only help in the rapid and early diagnosis of infection but also help in determining drug resistance,[rx] and include:
- Uniplex PCR for direct dermatophyte detection in clinical samples – A PCR for the direct detection of dermatophytes in skin scales is available as in-house PCR-ELISA assay which separately identifies numerous dermatophyte species. In a pilot study, the sensitivity and specificity of the test compared to cultures was 80.1% and 80.6%
- Multiplex PCR for fungal detection in dermatophytes – Commercially available multiplex PCR tests enable simultaneous amplification of 21 dermatomycotic pathogens with subsequent DNA detection by means of agarose gel electrophoresis.
New molecular methods like matrix-assisted laser desorption ionization-time of flight mass spectrometry
- It is based on the detection of biochemical characteristics, proteolytic degradation product which is a result of the activity of mycological infections or noninfectious diseases. These are represented by proteolytic degradation products of native proteins.
- The peptide patterns of affected samples are identified by comparison with known peptide spectra from skin disorders stored in an already existing database. This procedure is immensely time-saving, as it enables simultaneous identification of up to 64 dermatophyte strains, with results coming back within 24 h.[rx]
Reflectance confocal microscopy
- It provides imaging of the epidermis and superficial dermis at cellular level resolution and can be used to detect cutaneous fungi and parasitic infestations.[rx] Branching fungal hyphae can be detected over an erythematous annular scaly patch. The advantage of the test is noninvasive and in a retrospective analysis of the test by Friedman et al. sensitivity was found to be 100%.
Treatment for Paronychia
Non-Pharmacological
- Keeping the hands warm and dry – Avoiding anything which might irritate the skin, such as soaps and detergents. Also avoiding injury, eg avoid manicures, finger sucking, nail-biting, etc.
- Antiseptics or antifungal lotions – or solutions may be applied for several months. Topical antiseptic may be prescribed for a localized, minor infection.
- Draining the pus out – If a lot of pus has collected, and your finger or toe is very swollen, the pus may need to be drained. A small cut is made to allow the pus to come out.
- Warm bathing – It may also help to soak the affected finger in warm salted water four times a day. Soak affected digit in warm water, several times daily.
- Wear Comfortable shoes – Wearing very comfortable shoes if the affected nail is a toenail, to avoid any pressure on it.
- Tea tree oil – has been used as an alternative therapy for treating paronychia with some success. A study from 2002 reported that a 50 percent solution of tea tree oil effectively treated an athlete’s foot in 64 percent of trial participants.
- Treatment for paronychia which lasts more than six weeks – If the problem has dragged on for six weeks or more, it is called chronic paronychia. Chronic means persisting. If this is the case there may be an underlying skin condition. In other cases, there can be infected with a yeast or fungus. This is particularly common in those people mentioned above who have their hands in water a lot.
Pharmacological
- Antibiotics – If your infection is caused by bacteria then an antibiotic may be prescribed. Antibiotics commonly used for this type of infection include flucloxacillin or erythromycin. In a minor infection, an antibiotic cream may be all that is needed – for example, fusidic acid cream.
- NSAIDs – Prescription-strength drugs that reduce both pain and inflammation. Pain medicines and anti-inflammatory drugs help to relieve pain and stiffness, allowing for increased mobility and exercise. There are many common over-the-counter medicines called non-steroidal anti-inflammatory drugs (NSAIDs). They include etodolac, aceclofenac, etoricoxib, ibuprofen, and naproxen.
- Topical Medications – These prescription-strength creams, gels, ointments, patches, and sprays help relieve pain and inflammation through the skin.
- Calcium & vitamin D3 – To improve bone health and healing quickly. As a general rule, men and women age 50 and older should consume 1,200 milligrams of calcium a day, and 600 international units of vitamin D a day.
- Glucosamine & Diacerein, Chondroitin sulfate – can be used to tightening the loose tendon, cartilage, ligament, and cartilage, ligament regenerates cartilage or inhabits the further degeneration of cartilage, ligament.
- Dietary supplement -to remove general weakness & improved health.
- Antidepressants – A drug that blocks pain messages from your brain and boosts the effects of endorphins (your body’s natural painkillers).
- Vitamin C, Vitamin B complex and Vitamin E – It helps to heal the tissue, cell of the subcutaneous area and the infected side.
Treatment options include
- Topical corticosteroid ointment is applied for 2–4 weeks and repeated for flares.
- Tacrolimus ointment is an alternative when dermatitis is not responding to routine management.
- Intralesional steroid injections are sometimes used in resistant cases.
- Steroid creams, such as hydrocortisone or betamethasone.
- Antifungal creams such as clotrimazole, miconazole or terbinafine.
- Antifungal tablets such as terbinafine or itraconazole.
- An operation to open up the infected area, and keep it open and let it drain and heal over time.
Acute paronychia
- Oral antibiotics may be necessary for severe or prolonged bacterial infection; often a tetracycline such as doxycycline is prescribed.
- Consider early treatment with aciclovir in case of severe herpes simplex infection.
- Surgical incision and drainage may be required for abscess followed by irrigation and packing with gauze.
- Rarely, the nail must be removed to allow pus to drain.
- Oral antifungal agent (itraconazole or fluconazole), if C Albicans is confirmed.
Chronic paronychia
Attend to predisposing factors.
- Keep the hands dry and warm.
- Avoid wet work, or use totally waterproof gloves that are lined with cotton.
- Keep fingernails scrupulously clean.
- Wash after dirty work with soap and water, rinse off and dry carefully.
- Apply emollient hand cream frequently – dimethicone barrier creams may help.
Other management
- Patients with diabetes and vascular disease with toenail paronychia infections should be examined for signs of cellulitis.
- Surgical excision of the proximal nail fold may be necessary.
- Eponychial marsupialization involves surgical removal of a narrow strip of skin next to the nail, to reduce the risk of infection.
- Swiss roll technique has the advantage of retaining the nail plate and quicker recovery.
[stextbox id=’custom’]
Treatment Options for Typical Pathogens Associated with Acute Paronychia
| PATHOGEN | ANTIBIOTIC OPTIONS |
|---|---|
|
Gram-negative aerobes |
|
|
Fusobacterium |
Amoxicillin/clavulanate (Augmentin), clindamycin, fluoroquinolones |
|
Pseudomonas |
Ciprofloxacin |
|
Gram-negative anaerobe |
|
|
Bacteroides |
Amoxicillin/clavulanate, clindamycin, fluoroquinolones |
|
Gram-negative facultative anaerobes |
|
|
Eikenella |
Cefoxitin |
|
Enterococcus |
Amoxicillin/clavulanate |
|
Klebsiella |
Trimethoprim/sulfamethoxazole, fluoroquinolones |
|
Proteus |
Amoxicillin/clavulanate, fluoroquinolones |
|
Gram-positive aerobes |
|
|
Staphylococcus |
Cephalexin (Keflex) |
|
For suspected methicillin-resistant Staphylococcus aureus infections: clindamycin, doxycycline, trimethoprim/sulfamethoxazole |
|
|
Streptococcus |
Cephalexin |
note: Local community resistance patterns should always be considered when choosing antibiotics.
[/stextbox]
Prevention
Because fungi grow particularly well in a moist environment, it’s important to make sure you keep your feet dry. You might try the following, for example:
- Wash your feet with soap and water every day and dry them thoroughly, especially between the toes.
- Wash socks, bedding, and towels in water that’s 140°F (60°C) or higher. Combining washing socks and application of OTC antifungal recommendations should treat most cases of athlete’s foot. You can disinfect your shoes by using disinfectant wipes (like Clorox wipes) or sprays.
- Put antifungal powder on your feet every day.
- Don’t share socks, shoes, or towels with others.
- Wear sandals in public showers, around public swimming pools, and in other public places.
- Wear socks made out of breathable fibers, such as cotton or wool, or made out of synthetic fibers that wick moisture away from your skin.
-
Thoroughly dry your feet with a towel after having a shower or bath, or after swimming
-
Wearing shoes that aren’t too tight and let your feet breathe
-
Not wearing the same pair of shoes two days in a row
-
Taking your shoes off as often as possible
-
Dry feet and toes meticulously after bathing
-
Use desiccating foot powder once or twice daily
-
Avoid wearing occlusive footwear for long periods
-
Thoroughly dry shoes and boots
-
Clean the shower and bathroom floors using a product containing bleach
- Great shoes with antifungal powder. If treatment of tinea pedis is unsuccessful, consider reinfection, coexistent untreated fungal nail infection, reinfection due to an untreated family member, or an alternative diagnosis.
-
Wearing flip-flops when using swimming pools, communal showers and changing rooms
-
Not sharing towels, shoes, or socks
-
Washing socks, bedding, and towels at 60 degrees Celsius or more
-
Adding special anti-fungal laundry sanitizers if washing at lower temperatures
Can paronychia be prevented or avoided by
The best away to avoid acute paronychia is to take good care of your nails.
- Avoid injuring your nails and fingertips.
- Don’t bite or pick your nails.
- Keep your nails trimmed and smooth.
- Avoid cutting nails too short.
- Don’t scrape or trim your cuticles, as this can injure the skin.
- Use clean nail clippers or scissors.