Extruded Discs or disc extrusion, occur when the nucleus material of a spinal disc pushes completely through the outer edge of the disc or seeps into the spinal column. And, it can lead to lower back pain in many patients. In this post, we discuss the symptoms of disc extrusion as well as disc extrusion treatments (surgical and non-surgical) for relieving your pain.
Disc extrusions are caused by a weakened disc wall, or annulus fibrosus, rupturing due to age or injury. This outer wall is what keeps the soft, jelly-like center of the disc contained, creating a type of cushion for the vertebrae to bend and move freely. When a disc becomes ruptured or herniated, an annular tear occurs, allowing the jelly-like center to spill into the spinal cavity-causing irritation, inflammation, and pinched nerves.
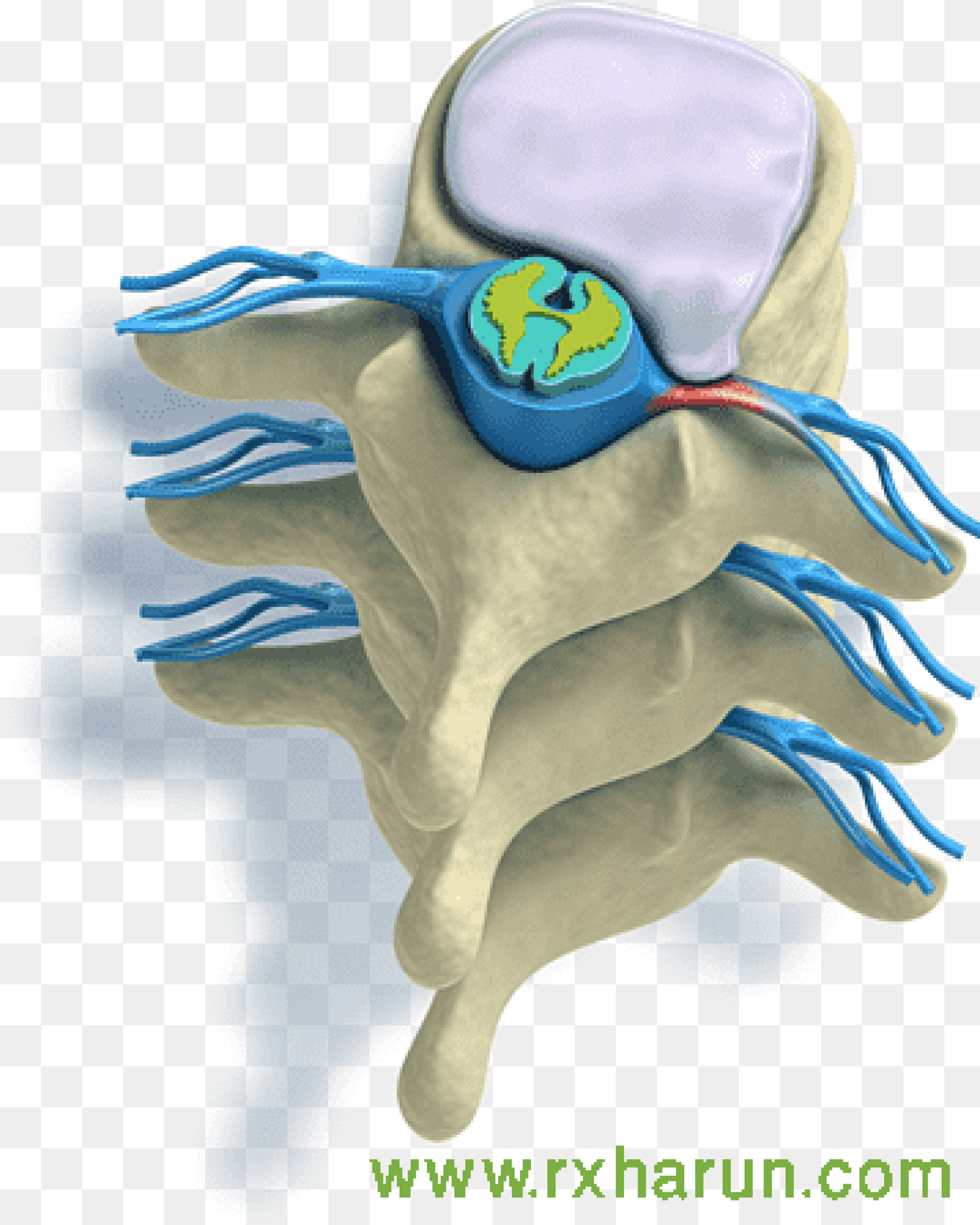
Disc Extrusion is a tear in the outermost layer of the spinal disc, causing spinal disc tissue to spill out. But the tissue that has come out is still connected to the disc.

Causes of Extruded Discs
- Disc herniation and disc extrusion – are associated terms, being nucleus pulposus herniation a possible evolution from a degenerative disc. A disc extrusion is usually associated with the loss of proteoglycans.[rx] Multiple factors influence the disc extrusion process such as genetic, mechanical, and behavioral.[rx][rx]
- Mechanical load – is important in maintaining a healthy IVD by generating signals to cells that regulate proper matrix homeostasis.[rx][rx] On the other hand, prolonged exposure to hypo- or hyper-loading correlates with disc extrusion induction.[rx][rx]
- Repetitive trauma – such as poor posture, poor ergonomics, or repetitive heavy work can lead to disc extrusion and a bulging disc. These long term injuries are often also associated with poor muscle strength, obesity, and other factors such as smoking.
- An Injury caused – by sudden forces or load on the disc such as a car accident or an awkward heavy lift. This sudden increase in pressure on the disc can cause damage and tears to the annulus that causes a disc extrusion.
- Spinal Degeneration – While some disc extrusion is a normal part of the aging process, poor spinal function and posture will dramatically speed up disc extrusion with a bulging disc.
- People who have led a sedentary lifestyle or those who smoke – increase the chances for bulging discs.
- Continuous strain on the disc from injury or heavy lifting – and strain can wear them down throughout the years.
- Weakened back muscles – can accelerate the process and may lead to a sudden herniation of the weakened disc. Although bulging discs occur over time, disc extrusion may occur quickly by trauma.
- Bad posture – including improper body positioning during sleep, sitting, standing, or exercise are all risk factors that may contribute to the development of disc extrusion.
- Obesity
- High contact sports or activities – are also risk factors.
- Runners who fail to use shoes that provide orthopedic support – may also develop disc extrusion.
- Activities that place stress and strain on the spine – can lead to the weakening of the discs.
Symptoms of Extruded Discs
If a disc extrusion has not yet reached the stage of herniation, a patient may have little to no pain involved. A disc extrusion may have no pain at all because it has not reached a certain severity level, and this can make it difficult to identify the disc extrusion symptoms before the condition becomes more severe.
Most commonly, disc extrusion creates pressure points on nearby nerves which create a variety of sensations. Evidence of a disc extrusion may range from mild tingling and numbness to moderate or severe pain, depending on the severity. In most cases, when a disc extrusion has reached this stage it is near or at herniation.
- Tingling or pain in the fingers, hands, arms, neck or shoulders – This could indicate a disc extrusion in the cervical area.
- Pain in the feet, thighs, lower spine and buttocks – This is the most common symptom and could indicate an issue in the lumbar region.
- Difficulty walking or feeling of impairment while lifting or holding things.
- Loss of Bladder or Bowel Function – There are some disc extrusion cases where professional care is essential. In some cases, such as when you lose bowel or bladder control, it is deemed an emergency, and you may require immediate surgery. These bulges usually are very significant and affect your nerve control involving your bladder or bowels. You should go straight to your nearest emergency department in these instances.
- Weakness in your limb muscles – is a significant concern. If you experience arm, hand, leg or foot weakness, please seek prompt medical assessment.
- The reduced or altered sensation – is your next priority. Mild disc extrusion can reduce your ability to feel things touching you, e.g. numbness or pins and needles. If you experience any of the above symptoms, you should seek professional assistance.
- Referred Pain – Pain in your limbs, e.g. legs (sciatica) or arms (brachialgia) is usually a more significant injury than when experiencing only spinal pain. We recommend that you seek the professional advice of your trusted spinal care practitioner.
- Spinal Pain – Interestingly, if you are only experiencing spinal pain, disc extrusions are generally mild injuries and the most likely to rehabilitate quickly. Please adhere to low disc pressure postures and exercise accordingly. If in doubt, please seek professional advice.
- Intermittent or continuous back pain. This may be made worse by movement, coughing, sneezing, or standing for long periods of time.
- Spasm of the back muscles
- Sciatica. Pain that starts near the back or buttock and travels down the leg to the calf or into the foot.
- Muscle weakness in the legs
- Numbness in the leg or foot
- Decreased reflexes at the knee or ankle
- Changes in bladder or bowel function
Associate clinical feature is
- Severe back pain
- Saddle anesthesia i.e., anesthesia or paraesthesia involving S3 to S5 dermatomes, including the perineum, external genitalia, and anus; or more descriptively, numbness or “pins-and-needles” sensations of the groin and inner thighs which would contact a saddle when riding a horse.
- Bladder and bowel dysfunction, caused by a decreased tone of the urinary and anal sphincters.
- Detrusor weaknesses causing urinary retention and post-void residual incontinence as assessed by bladder scanning the patient after the patient has urinated.
- Sciatica type pain on one side or both sides, although pain may be wholly absent
- The weakness of the muscles of the lower legs (often paraplegia)
- Pain in one leg (unilateral) or both legs (bilateral) that starts in the buttocks and travels down the back of the thighs and legs (sciatica)
- Numbness in the groin or area of contact if sitting on a saddle (perineal or saddle paresthesia)
- Bowel and bladder disturbances
- Lower extremity muscle weakness and loss of sensations
- Inability to urinate (urinary retention)
- Difficulty initiating urination (urinary hesitancy)
- The decreased sensation when urinating (decreased urethral sensation)
- Inability to stop or control urination (incontinence)
- Reduced or absent lower extremity reflexes
- Local pain is generally a deep, aching pain resulting from soft tissue and vertebral body irritation.
- Leg pain (radicular pain) is generally a sharp, stabbing pain resulting from compression of the nerve roots.
- Radicular pain projects along with the specific areas controlled by the compressed nerve (known as a dermatomal distribution).
- Inability to stop or feel a bowel movement (incontinence)
- Constipation
- Loss of anal tone and sensation
- Achilles (ankle) reflex absent on both sides.
- Sexual dysfunction
- Absent anal reflex and bulbocavernosus reflex
- Gait disturbance
These symptoms require immediate medical evaluation as they may be a sign of a potentially life-threatening condition.
Diagnosis of Disc Extrusion
History
Proper understanding of anatomical zones and vertebral levels is essential to interpret the clinical manifestations secondary to a disc extrusion. Wiltse proposed these anatomical zones, based on the following landmarks: medial border of the articular facet, lateral, upper, and medial borders of the pedicles, coronal and sagittal planes at the center of the disc. On the axial plane, these landmarks determine the central zone, the subarticular zone (lateral recess), foraminal, and extraforaminal zones. On the sagittal plane, the levels are termed as follows: The supra pedicular level, the pedicular level, the intravesicular level, and the disc level. The correct knowledge of anatomy and the relationship between nerve roots and disc herniation allows the proper understanding of common clinical findings associated with this problem.
We summarize the anatomy, motor function, sensitive distribution, and reflex of the most commons nerve roots involved in cervical and lumbosacral nucleus pulposus herniation:
Cervical
-
C5 nerve root – Exits between C4 and C5 foramina, innervates deltoids and biceps (with C6), sensory distribution: lateral arm (axillary nerve) and is assessed with biceps reflex.
-
C6 nerve root – Exits between C5 and C6 foramina, innervates biceps (with C5) and wrist extensors, sensory distribution: lateral forearm (musculocutaneous nerve), assessed with brachioradialis reflex.
-
C7 nerve root – Exits between C6 and C7 foramina, innervates triceps, wrist flexors, and finger extensors, sensory distribution: middle finger, assessed with triceps reflex.
-
C8 nerve root – Exits between C7 and T1 foramina, innervates interosseus muscles and finger flexors, sensory distribution: ring and little fingers and distal half of the forearm (ulnar side), no reflex.
Lumbosacral
-
L1 nerve root – Exits between L1 and L2 foramina, innervates iliopsoas muscle, sensory distribution: upper third thigh, assessed with the cremasteric reflex (male).
-
L2 nerve root – Exits between L2 and L3 foramina, innervates iliopsoas muscle, hip adductor, and quadriceps, sensory distribution: middle third thigh, no reflex.
-
L3 nerve root – Exits between L3 and L4 foramina, innervates iliopsoas muscle, hip adductor, and quadriceps, sensory distribution: lower third thigh, no reflex.
-
L4 nerve root – Exits between L4 and L5 foramina, innervates quadriceps and tibialis anterior, sensory distribution: anterior knee, medial side of the leg, assessed with patellar reflex.
-
L5 nerve root – Exits between L5 and S1 foramina, innervates extensor hallucis longus, extensor digitorum longus, and Brevis, and gluteus medius, sensory distribution: anterior leg, lateral leg, and dorsum of the foot, no reflex.
-
S1 Nerve – back, radiating into buttock, lateral or posterior thigh, posterior calf, lateral or plantar foot; sensory loss on the posterior calf, lateral or plantar aspect of foot; weakness on hip extension, knee flexion, plantar flexion of the foot; Achilles tendon; Medial buttock, perineal, and perianal region; weakness may be minimal, with urinary and fecal incontinence as well as sexual dysfunction.
-
S2-S4 Nerves – sacral or buttock pain radiating into the posterior aspect of the leg or the perineum; sensory deficit on the medial buttock, perineal, and perianal region; absent bulbocavernosus, anal wink reflex.
Cervical and thoracic disc herniation can also exhibit symptoms of myelopathy such as spasticity, clumsiness, wide-based gate, and weakness, on physical examination hyperreflexia is the most important sign. The Lhermitte sign is the presence of an electric shock-like sensation towards the back and lower extremities, especially by flexing the neck.[rx][rx] Bowel and bladder dysfunction may indicate a poor prognosis.
Physical Examination
A physical exam for diagnosing disc pain may include one or more of the following tests:
- Palpation – Palpating (feeling by hand) certain structures can help identify the pain source. For example, worsened pain when pressure is applied to the spine may indicate sensitivity caused by a disc extrusion.
- Movement tests – Tests that assess the spine’s range of motion may include bending the neck or torso forward, backward, or to the side. Additionally, if raising one leg in front of the body worsens leg pain, it can indicate a disc extrusion (straight leg raise test).
- Muscle strength – A neurological exam may be conducted to assess muscle strength and determine if a nerve root is compressed by a disc extrusion. A muscle strength test may include holding the arms or legs out to the side or front of the body to check for tremors, muscle atrophy, or other abnormal movements.
- Reflex test – Nerve root irritation can dampen reflexes in the arms or legs. A reflex test involves tapping specific areas with a reflex hammer. If there is little or no reaction, it may indicate a compressed nerve root in the spine.
- The straight leg raise test – With the patient lying supine, the examiner slowly elevates the patient’s led at an increasing angle, while keeping the leg straight at the knee joint. The test is positive if it reproduces the patient’s typical pain and paresthesia.[rx]
- The contralateral (crossed) straight leg raise test – As in the straight leg raise test, the patient is lying supine, and the examiner elevates the asymptomatic leg. The test is positive if the maneuver reproduces the patient’s typical pain and paresthesia. The test has a specificity higher than 90%.
Lab Test
- A medical history – in which you answer questions about your health, symptoms, and activity.
- Erythrocyte sedimentation rate and C-reactive protein – are inflammatory markers, and they are requested if suspicious for a chronic inflammatory condition or infectious cause as the etiology. A complete blood count is useful when suspecting infection or malignancy.
- A physical exam to assess your strength – reflexes, sensation, stability, alignment, and motion. You may also need blood tests.
- Elevated ESR – could indicate infection, malignancy, chronic disease, inflammation, trauma, or tissue ischemia.
- Elevated CRP – levels are associated with infection.
Imaging
- X-rays – X-ray is the initial workup study when there is a strong suspicion of a specific cause of cervical or back pain (fracture, infection, tumor) or in the presence of red flags (fever, age more than 50, recent trauma, pain at night or rest, unexplained weight loss, progressive motor or sensory deficit, saddle anesthesia, history of cancer or osteoporosis, failure to improve after six weeks of conservative treatment). Anteroposterior and lateral x-ray is helpful to assess fracture, bony deformity, decreased intervertebral height, osteophytes, spondylolisthesis, and facet joint osteoarthritis and disc extrusion.
- Magnetic Resonance Imaging (MRI) scan – MRI is the recommended diagnostic imaging in cases of severe or progressive neurologic deficits, suspicion of an underlying condition such as infection, fracture, cauda equina syndrome, spinal cord compression. In cases of radiculopathy, most of the cases improve with conservative treatment and MRI is indicated in those cases with significant pain or neurologic deficits.[rx]
- A myelogram – is a specialized X-ray where dye is injected into the spinal canal through a spinal tap. An X-ray fluoroscope then records the images formed by the dye. The dye used in a myelogram shows up white on the X-ray, allowing the doctor to view the spinal cord and canal, a bulging disc in detail. Myelograms can show a nerve being pinched and a bulging disc by a herniated disc, bony overgrowth, spinal cord tumors, and abscesses. A CT scan may follow this test.
- Computed Tomography (CT) scan – is a noninvasive test that uses an X-ray beam and a computer to make 2-dimensional images of your spine. It may or may not be performed with a dye (contrast agent) injected into your bloodstream. This test is especially useful for confirming which bulging disc is damaged. CT scan is not usually requested in nucleus pulposus herniation. However, it can be helpful in some cases when there is a suspicion of calcified disc herniation (thoracic disc herniation has a 30 to 70% rate of calcification) which is more challenging especially when surgery is a consideration.
- Electromyography (EMG) & Nerve Conduction Studies (NCS) – EMG tests measure the electrical activity of your muscles. Small needles are placed in your muscles, and the results are recorded on a special machine. NCS is similar, but it measures how well your nerves pass an electrical signal from one end of the nerve to another. These tests can detect nerve damage and muscle weakness and a bulging disc.
- Discogram – A discogram may be recommended to confirm which bulging disc is painful if surgical treatment is considered. In this test, the radiographic dye is injected into the disc to recreate disc pain from the dye’s added pressure.
Treatment of Disc Extrusion
Non-Surgical
- Spine-Specialized physical therapy – typically includes a combination of stretching, strengthening, and aerobic exercise to provide better stability and support for the spine.
- Massage therapy – can help reduce muscle tension and muscle spasms, which may add to back or neck pain. Muscle tension is especially common around an unstable spinal segment where a disc is unable to provide the necessary support
- Ice & Moist Heat Application – Ice application where the ice is wrapped in a towel or an ice pack for about 20 minutes to the affected region, thrice a day, helps in relieving the symptoms of a disc bulge. Heat application in the later stages of treatment also provides the same benefit.
- Hot Bath – Taking a hot bath or shower also helps in dulling the pain from a disc bulge. Epsom salts or essential oils can be added to a hot bath. They will help in soothing the inflamed region.
- Traction – traction is the best essential treatment for bulging discs, pinched nerve, radiating pain management. It can be done in a manual and dynamic way to relieves pain in bulging discs.
- Massage therapy – may give short-term pain relief, but not functional improvement, for those with acute lower back pain. It may also give short-term pain relief and functional improvement for those with long-term (chronic) and sub-acute lower back pain, but this benefit does not appear to be sustained after 6 months of treatment. There does not appear to be any serious adverse effects associated with massage.
- Acupuncture – may provide some relief for back pain. However, further research with stronger evidence needs to be done.
- Spinal manipulation – is a widely-used method of treating back pain, although there is no evidence of long-term benefits.
- Back school – is an intervention that consists of both education and physical exercises. A 2016 Cochrane review found the evidence concerning back school to be very low quality and was not able to make generalizations as to whether the back school is effective or not.
- Patient education – on proper body mechanics (to help decrease the chance of worsening pain or damage to the disk)
- Physical therapy – which may include ultrasound, massage, conditioning, and exercise. The goal of physical therapy is to help you return to full activity as soon as possible and prevent re-injury. Physical therapists can instruct you on proper posture, lifting, and walking techniques, and they’ll work with you to strengthen your lower back, leg, and stomach muscles. They’ll also encourage you to stretch and increase the flexibility of your spine and legs. Exercise and strengthening exercises are key elements to your treatment and should become part of your life-long fitness.
- Over the Door Traction – This is a very effective treatment for a disc bulge. It helps in relieving muscle spasms and pain. Typically a 5 to 10-pound weight is used and it is important that patients do this under medical guidance.
- Weight control – By keto diet or maintaining or changing the food habit to reduce the weight not any movement during the time of acute pain.
- Use of lumbosacral back support – It is helpful for back support during any travels or everyday natural movement. It also helps to straighten the lumbar spine.
- Typically – conservative therapy is the first line of treatment to manage lumbar disk disease. Approach for Treating and Reversing a Disc Bulge about half of the disc bulges heal within six months and only about 10% of the disc bulges require surgery. So, the good news is that conservative treatment for a disc bulge helps in treating as well as reversing the disc bulges.
- Eat Nutritiously During Your Recovery – All bones and tissues in the body need certain nutrients in order to heal properly and in a timely manner. Eating a nutritious and balanced diet that includes lots of minerals and vitamins are proven to help heal back pain of all types. Therefore focus on eating lots of fresh produce (fruits and veggies), whole grains, lean meats, and fish to give your body the building blocks needed to properly healing PLID. In addition, drink plenty of purified water, milk, and other dairy-based beverages to augment what you eat.
- In bulging disc needs ample minerals (calcium, phosphorus, magnesium, boron) and protein to become strong and healthy again.
- Excellent sources of minerals/protein include dairy products, tofu, beans, broccoli, nuts and seeds, sardines, and salmon.
- Important vitamins that are needed for bone healing include vitamin C (needed to make collagen), vitamin D (crucial for mineral absorption), and vitamin K (binds calcium to bones and triggers collagen formation).
- Conversely, don’t consume food or drink that is known to impair bone/tissue healing, such as alcoholic beverages, sodas, most fast food items, and foods made with lots of refined sugars and preservatives.
Medications
- Acetaminophen (paracetamol) – Acetaminophen (paracetamol) is also a painkiller, but it is not an NSAID. It is well tolerated and can be used as an alternative to NSAIDs – especially for people who do not tolerate NSAID painkillers because of things like stomach problems or asthma. But higher doses of acetaminophen can cause liver and kidney damage. For this reason, adults should follow the information on the package insert and make sure they do not take more than 4 grams (4,000 milligrams) of acetaminophen per day. This is the amount in, for example, 8 tablets containing 500 milligrams each. It is not only important to take the right dose, but also to wait long enough between doses.
- Muscle Relaxants – These medications provide relief from spinal muscle spasms. Muscle relaxants, such as baclofen, tolperisone, eperisone, methocarbamol, carisoprodol, and cyclobenzaprine, may be prescribed to control muscle spasms. Sedatives also relax the muscles. Like other psychotropic medications, they can cause fatigue and drowsiness, and affect your ability to drive. Muscle relaxants can also affect the functioning of your liver and cause gastrointestinal (stomach and bowel) complications. Benzodiazepines such as tetrazepam may lead to dependency if they are taken for longer than two weeks.
- Neuropathic Agents – Drugs(pregabalin & gabapentin) that address neuropathic—or nerve-related—pain. This includes burning, numbness, and tingling.
- Opioids – Also known as narcotics, these medications are intense pain relievers that should only be used under a doctor’s careful supervision. Strong painkillers that may only be used under medical supervision. Opioids are available in many different strengths, and some are available in the form of a patch. Morphine, for example, is a very strong drug, while tramadol is a weaker opioid.
- NSAIDs – Prescription-strength drugs that reduce both pain and inflammation. Pain medicines and anti-inflammatory drugs help to relieve pain and stiffness, allowing for increased mobility and exercise. There are many common over-the-counter medicines called non-steroidal anti-inflammatory drugs (NSAIDs). They include mainly or first choice etodolac, then aceclofenac, etoricoxib, ibuprofen, and naproxen.
- Calcium & vitamin D3 – To improve bone health and healing fracture. As a general rule, men and women age 50 and older should consume 1,200 milligrams of calcium a day, and 600 international units of vitamin D a day.
- Glucosamine & Diacerein, Chondroitin sulfate – can be used to tightening the loose tendon, cartilage, ligament, and cartilage, ligament regenerates cartilage or inhabits the further degeneration of cartilage, ligament.
- Dietary supplement – to remove general weakness & improved health.
- Vitamin B1, B6, and B12 – It is essential for neuropathic pain management, pernicious anemia, with vitamin b complex deficiency pain, paresthesia, numbness, itching with diabetic neuropathy pain, myalgia, etc.
- Antidepressants – A drug that blocks pain messages from your brain and boosts the effects of endorphins (your body’s natural painkillers).
- Corticosteroid – to healing the nerve inflammation and clotted blood in the joints. Steroids may be prescribed to reduce the swelling and inflammation of the nerves. They are taken orally (as a Medrol dose pack) in a tapering dosage over a five-day period. It has the advantage of providing almost immediate pain relief within a 24-hour period.
-
Anticonvulsants – These medications are typically used to treat epilepsy, but some are approved for treating nerve pain (neuralgia). Their side effects include drowsiness and fatigue. This can affect your ability to drive.
- Topical Medications – These prescription-strength creams, gels, ointments, patches, and sprays help relieve pain and inflammation throughout the skin.
- Steroid injections The procedure is performed under x-ray fluoroscopy and involves an injection of corticosteroids and a numbing agent into the epidural space of the spine. The medicine is delivered next to the painful area to reduce the swelling and inflammation of the nerves. About 50% of patients will notice relief after an epidural injection, although the results tend to be temporary. Repeat injections may be given to achieve the full effect. Duration of pain relief varies, lasting for weeks or years. Injections are done in conjunction with physical therapy and/or a home exercise program.
Surgery
- Microdiscectomy – for a herniated disc, a minimally-invasive procedure in which the herniated portion of the disc is removed.
- Artificial disc replacement – for degenerative disc disease and herniated discs is a minimally invasive procedure that replaces a damaged disc with a specialized implant that mimics the normal function of the disc, maintaining mobility.
- Spinal fusion – fusion for degenerative disc disease, in which the disc space is fused together to remove motion at the spinal segment. Spinal fusion involves setting up a bone graft, as well as possible implanted instruments, to facilitate bone growth across the facet joints. Fusion occurs after the surgery.
- Open Back Surgery – Traditionally, bulging discs are treated with an open back procedure, meaning the surgeon makes a large incision into the skin and cuts muscle and surrounding tissue to gain access to the problematic disc. This traditional surgical option is invasive, requires overnight hospitalization, general anesthesia, and requires a lengthy recovery coupled with strong pain medication.
- Endoscopic Surgery – Fortunately, you have a second option with endoscopic spine surgery. Thanks to the advancement of surgical technology at bulged disc surgery can be performed using endoscopic procedures, meaning the surgeon makes a small incision to insert special surgical tools. During an endoscopic bulging disc operation, the surgeon uses a tiny camera to visualize and gain access to your damaged disc. This minimally invasive new approach offers shorter recovery, easier rehabilitation, and a much higher success rate than open back or neck surgery. A local anesthetic is all that is usually required.
- Total Disc Replacement (TDR) and Anterior Cervical Discectomy and Fusion (ACDF) – Surgical exposure of the desired vertebral level is achieved through an anterior cervical incision. Subcutaneous dissection is performed to allow for adequate mobilization to tissue incision. The discectomy is performed with pituitary rongeurs, curette, and a burr drill to remove the affected disc. The posterior longitudinal ligament can be left in situ depending on the severity of the herniation. The center of the disc is identified. A keel is made using the burr after which the disc is removed and disc replacement performed. A similar surgical method is used for anterior cervical discectomy and fusion, the difference is the type of implant, which can be an interbody cage with an anterior cervical plate or a standalone cage. Although complications are rare, patients experience dysphagia, hoarseness, and transient sore throat. Adjacent segment disease or pseudoarthrosis can occur depending on severity and number of levels operated. The majority of patients get symptomatic relief and can resume full activity after six months.
- Laminectomy – Cervical laminectomy removes the lamina on one or both sides to increase the axial space available for the spinal cord. Clinically indicated for spinal stenosis or cervical disc disease involving more than three levels of disc degeneration with anterior spinal cord compression. Single-level cervical disc herniation is usually managed with the anterior approach. The complications of the posterior approach include instability resulting in kyphosis, recalcitrant myofascial pain, and occipital headaches.
- Laminoplasty – The kyphotic deformity is a well-known complication of laminectomy. To preserve the posterior wall of the spinal canal while decompressing the spinal canal a Z-plasty technique for the lamina was developed. The variant of the procedure uses a hinged door for the lamina. Laminoplasty is commonly indicated for multilevel spondylotic myelopathy. Nerve root injury is seen in about 11% of the surgeries. This complication is unique to laminoplasty, and the suggested etiology is traction on the nerve root with the posterior migration of the spinal cord.
Some patients will not benefit from conservative treatment and will require surgery to decompress the nerve involved. Classical surgical indications are motor deficit, cauda equina syndrome, and persistent pain after conservative treatment.[rx]
Anticonvulsants and antidepressants are typically not used unless the symptoms last for a longer period of time or the painkillers don’t provide enough relief.
References