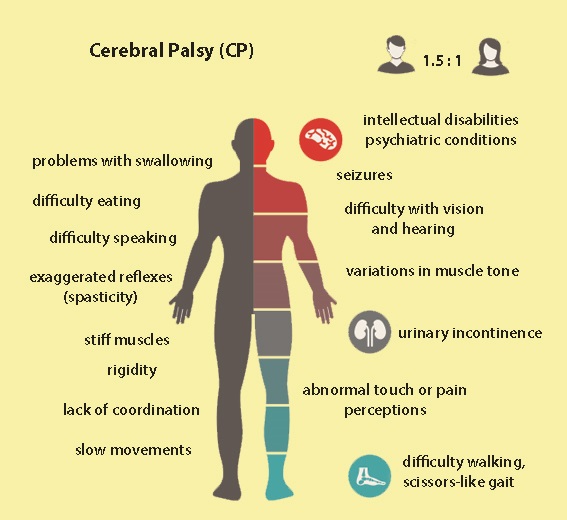
Cerebral Palsy is a group of neurological non-progressive/ permanent movement disorders that appear in early childhood or before, during, or after birth due to brain injury or abnormal development of the brain or injury of the brain & central nervous system. Often, symptoms include poor coordination, stiff muscles, weak muscles, tre, more, and maybe problems with sensation, vision, hearing, swallowing, and speaking.
Cerebral palsy is a broad range of static, non-progressive motor disabilities that present from birth or early childhood as a result of injury to neuromotor components of the central nervous system. Motor performance is normally coordinated via communication between the cerebral cortex, thalamus, basal ganglia, brain stem, cerebellum, and spinal cord, and communicating sensory-motor pathways. This complex network lends itself to injury at many different levels. Etiologies are numerous and can occur during the prenatal, perinatal, and postnatal periods. The severity of the neurologic deficit and the clinical manifestations are varied depending on the time, location, and nature of the original injury. To approach cerebral palsy systematically, the primary health care practitioner must be prepared to recognize neuromotor deficits, diagnose and classify the type of disorder, and implement a methodical treatment plan. The purpose of this article is to review the etiology, pathophysiology, diagnostic classification (Swedish system), clinical manifestations, and therapeutic management of cerebral palsy and prepare the advanced practice nurse to care for the individual and family.
Types of Cerebral Palsy
Geographical classification of cerebral palsy.
Major types
Description
Monoplegia
One extremity involved, usually a lower
Hemiplegia (30%)
Both extremities on the same side involved
Usually, the upper extremity is involved more than the lower extremity
Paraplegia
Both lower extremities are equally involved
Diplegia (50%)
The lower extremities more involved than the upper extremities
Fine motor/sensory abnormalities in the upper extremity
Velocity-dependent increase in muscle tone with passive stretch
Joint contractures are common
Athetoid
Dyskinetic, purposeless movements
Joint contractures are uncommon
Dystonia or hypotonia can be associated
Choreiform
Continual purposeless movements
Rigid
Hypertonicity occurs in the absence of hyperreflexia, spasticity, and clonus
Cogwheel” or “lead pipe” muscle stiffness
Ataxic
Disturbance of coordinated movement, most commonly walking
Normal head/neck control
Hypotonic
Low muscle tone and normal deep tendon reflexes
Mixed
Features of more than one type
No head/neck control
Cerebral Palsy Classification Levels
To classify how cerebral palsy affects your child’s physical abilities. we most often use these scales:
The Gross Motor Function Classification System – Expanded & Revised (GMFCS–E&R) – includes categories that describe the ability to walk, run and perform other large motor skills. The higher the GMFCS level, the more difficulty your child has performed such skills.
The Manual Ability Classification System (MACS) – includes categories that describe the ability to manipulate objects with the hands. The higher the MACS level, the more difficulty your child has performed such skills.
Physiologically, cerebral palsy can be divided into a spastic type, which affects the corticospinal (pyramidal) tracts, and an extrapyramidal type, which affects the other regions of the developing brain. The extrapyramidal types of cerebral palsy include athetoid, choreiform, ataxia, rigid, and hypotonic.
Gross Motor Function Classification System – Expanded & Revised (GMFCS–E&R)
The GMFCS uses five classification levels to describe the gross motor function of kids and teens who have cerebral palsy. The criteria for being classified within a particular level are based on functional abilities and depend on your child’s age—in general, classification is determined by the primary method of mobility your child uses after age 6. These are the descriptions for ages 12 to 18:
Level I
Walk at home, school, outdoors, and in the community.
Able to climb curbs and stairs without physical assistance or a railing.
Can run and jump but speed, balance, and coordination are limited.
Level II
Walk-in most settings but environmental factors and personal choice influence mobility choices.
Might require a hand-held mobility device for safety at school or work and climb stairs holding onto a railing.
Might use wheeled mobility when traveling long distances outdoors and in the community.
Level III
Capable of walking using a hand-held mobility device.
Might climb stairs holding onto a railing with supervision or assistance.
Might self-propel a manual wheelchair or use powered mobility at school.
Use powered mobility or be transported in a wheelchair outdoors and in the community.
Level IV
Use wheeled mobility in most settings.
Require physical assistance from one to two people for transfers
Might walk short distances indoors with physical assistance; use wheeled mobility or a body support walker when positioned.
Might operate a powered chair, otherwise are transported in a manual wheelchair.
Level V
Are transported in a manual wheelchair in all settings.
Limited in the ability to maintain antigravity head and trunk postures and control leg and arm movements.
Self-mobility is severely limited, even with the use of orthotics, prosthetics, and seating.
Manual Ability Classification System (MACS)
The MACS includes five levels that describe the ability of children (ages 4 to 18) to use their hands and handle objects.
Level I
Handles objects easily and successfully.
Experiences limitations in performing manual tasks requiring speed and accuracy. (These limitations don’t interfere with independence in daily activities.)
Level II
Handles most objects, but with reduced quality and/or speed in achieving tasks and activities.
Struggles with some activities; might need alternative ways of doing tasks. (These limitations usually don’t interfere with independence in daily activities.)
Level III
Handles objects with difficulty.
Needs help to prepare or adapt activities.
Does tasks slowly.
Experiences limited success regarding the quality and quantity of tasks and activities.
Performs activities independently only if they have been set up or adapted.
Level IV
Handles a limited selection of easily managed objects in adapted situations.
Performs only parts of activities with effort and limited success.
Requires continuous assistance and/or adapted equipment to attempt an activity.
Level V
Cannot handle objects.
Experiences severely limited the ability to perform even simple actions.
Requires total assistance.
Visit the MACS online resource site for more information.
Gross Motor Function Classification System (GMFC system)[rx] (RX)
GMFC system of cerebral palsy and approximate percentage in each group.
I
Has nearly normal gross motor function – 35%
II
Walks independently, but has limitations with running and jumping – 16%
III
Uses assistive devices to walk and wheelchair for long distances – 14%
IV
Has the ability to stand for transfers, but minimal walking ability; depends on a wheelchair for mobility – 16%
V
Lacks head control, cannot sit independently, is dependent on all aspects of care – 18%
The Topography of Cerebral Palsy
Hemiparesis (hemiplegia)—(predominantly) unilateral impairment of arm and leg on the same side
Diplegia—motor impairment primarily of the legs (usually with some relatively limited involvement of arms)
Triplegia—three-limb involvement
Quadriplegia (tetraplegia)—all four limbs, in fact, the whole body, are functionally compromised
European classification of (motor impairment in) cerebral palsy[rx]
Spastic cerebral palsy is characterized by at least two of
The abnormal movement pattern of posture or movement
Increased tone (not necessarily constant)
Pathological reflexes (increased reflexes, hyperreflexia, or pyramidal signs—for example, Babinski response)
Spastic bilateral cerebral palsy is diagnosed if
Limbs on both sides of the body are involved
Spastic unilateral cerebral palsy is diagnosed if
Limbs on one side of the body are involved
Ataxic cerebral palsy is characterized by both
The abnormal pattern of posture and/or movement
Loss of orderly muscular coordination so that movements are performed with abnormal force, rhythm, and accuracy
Dyskinetic cerebral palsy is dominated by both
The abnormal pattern of posture or movement
Involuntary, uncontrolled, recurring, and occasionally stereotyped movements
Dystonic cerebral palsy is dominated by both
Hypokinesia (reduced activity—stiff movement)
Hypertonia (tone usually increased)
Choreoathetotic cerebral palsy is dominated by both
Hyperkinesia (increased activity—stormy movement)
Hypotonia (tone usually decreased)
The severity of cerebral palsy: gross motor function classification system (for children between 6 and 12 years)[rx]
Level I—Walks without restrictions; limitations in more advanced gross motor skills
Level II—Walks without devices; limitations in walking outdoors and in the community
Level III—Walks with mobility devices; limitations in walking outdoors and in the community
Level IV—Self-mobility with limitations; children are transported or use power mobility outdoors and in the community
Level V—Self-mobility is severely limited even with the use of supporting technology
www.rxharun.com
The specific forms of cerebral palsy are determined by the extent, type, and location of a child’s abnormalities. Doctors classify CP according to the type of movement disorder involved — spastic (stiff muscles), athetoid (writhing movements), or ataxic (poor balance and coordination) — plus any additional symptoms, such as weakness (paresis) or paralysis (plegia). For example, hemiparesis (Hemi = half) indicates that only one side of the body is weakened. Quadriplegia (quad = four) means all four limbs are affected.
Spasticcerebral palsy – is the most common type of disorder. People have stiff muscles and awkward movements. Forms of spastic cerebral palsy include:
Spastic hemiplegia/hemiparesis – typically affects the arm and hand on one side of the body, but it can also include the leg. Children with spastic hemiplegia generally walk later and on tip-toe because of tight heel tendons. The arm and leg of the affected side are frequently shorter and thinner. Some children will develop an abnormal curvature of the spine (scoliosis). A child with spastic hemiplegia may also have seizures. The speech will be delayed and, at best, maybe competent, but intelligence is usually normal.
Spastic diplegia/diparesis – involves muscle stiffness that is predominantly in the legs and less severely affects the arms and face, although the hands may be clumsy. Tendon reflexes in the legs are hyperactive. The toes point up when the bottom of the foot is stimulated. Tightness in certain leg muscles makes the legs move like the arms of a scissor. Children may require a walker or leg braces. Intelligence and language skills are usually normal.
Spastic quadriplegia/quadriparesis– is the most severe form of cerebral palsy and is often associated with moderate-to-severe intellectual disability. It is caused by widespread damage to the brain or significant brain malformations. Children will often have severe stiffness in their limbs but floppy necks. They are rarely able to walk. Speaking and being understood is difficult. Seizures can be frequent and hard to control.
Dyskineticcerebral palsy (also includes athetoid, choreoathetosis, and dystonic cerebral palsies) – is characterized by slow and uncontrollable writhing or jerky movements of the hands, feet, arms, or legs. Hyperactivity in the muscles of the face and tongue makes some children grimace or drool. They find it difficult to sit straight or walk. Some children have problems hearing, controlling their breathing, and/or coordinating the muscle movements required for speaking. Intelligence is rarely affected in these forms of cerebral palsy.
Athetoid – Athetoid cerebral palsy or dyskinetic cerebral palsy (sometimes abbreviated ADCP) is primarily associated with damage to the basal ganglia in the form of lesions that occur during brain development due to bilirubin encephalopathy and hypoxic-ischemic brain injury. ADCP is characterized by both hypertonia and hypotonia, due to the affected individual’s inability to control muscle tone. Clinical diagnosis of ADCP typically occurs within 18 months of birth and is primarily based on motor function and neuroimaging techniques. Athetoid dyskinetic cerebral palsy is a non-spastic, extrapyramidal form of cerebral palsy. Dyskinetic cerebral palsy can be divided into two different groups; choreoathetosis and dystonic. Choreoathetotic CP is characterized by involuntary movements most predominantly found in the face and extremities. Dystonic ADCP is characterized by slow, strong contractions, which may occur locally or encompass the whole body.
Ataxiccerebral palsy – affects balance and depth perception. Children with ataxic CP will often have poor coordination and walk unsteadily with a wide-based gait. They have difficulty with quick or precise movements, such as writing or buttoning a shirt, or a hard time controlling voluntary movements such as reaching for a book.
Mixed types – of cerebral palsy refer to symptoms that don’t correspond to any single type of CP but are a mix of types. For example, a child with mixed CP may have some muscles that are too tight and others that are too relaxed, creating a mix of stiffness and floppiness.
Causes of Cerebral Palsy
Muscle control takes place in a part of the brain called the cerebrum. The cerebrum is the upper part of the brain. Damage to the cerebrum before, during, or within 5 years of birth can cause cerebral palsy.
The cerebrum is the upper part of the human brain.
The cerebrum is also responsible for memory, the ability to learn, and communication skills. This is why some people with cerebral palsy have problems with communication and learning. Cerebrum damage can sometimes affect vision and hearing.
Some newborns are deprived of oxygen during labor and delivery. In the past, it was thought that this lack of oxygen during birth led to brain damage.
However, during the 1980s, research showed that fewer than 1 in 10 cases of cerebral palsy stem from oxygen deprivation during birth. Most often, the damage occurs before birth, probably during the first 6 months of pregnancy.
There are at least three possible reasons for this.
Periventricular leukomalacia (PVL)
PVL is a kind of damage that affects the brain’s white matter because of a lack of oxygen in the womb. It may occur if the mother has an infection during pregnancy, such as rubella or German measles, low blood pressure, preterm delivery, or if she uses an illegal drug.
Abnormal development of the brain
Disruption of brain development can affect the way the brain communicates with the body’s muscles and other functions. During the first 6 months of pregnancy, the brain of the embryo or fetus is particularly vulnerable. Damage can stem from mutations in the genes responsible for brain development, certain infections such as toxoplasmosis, a parasite infection, herpes and herpes-like viruses, and head trauma.
Intracranial hemorrhage
Sometimes, bleeding inside the brain happens when a fetus experiences a stroke. Bleeding in the brain can stop the supply of blood to vital brain tissue, and this tissue can become damaged or die. The escaped blood can clot and damage surrounding tissue.
Several factors can cause a stroke in a fetus during pregnancy
A blood clot in the placenta blocks the flow of blood
A clotting disorder in the fetus
Interruptions in arterial blood flow to the fetal brain
Untreated pre-eclampsia in the mother
Inflammation of the placenta
Pelvic inflammatory infection in the mother
During delivery, the risk is increased by the following factors:
Emergency cesarean
The second stage of labor is prolonged
Vacuum extraction is used during delivery
Fetal or neonatal heart anomalies
Umbilical cord abnormalities
Anything that increases the risk of preterm birth or low birth weight also raises the risk of cerebral palsy.
Factors that may contribute to a higher risk of cerebral palsy include:
Multiple births, for example, twins
Damaged placenta
Sexually transmitted infections (STIs)
Consumption of alcohol, illegal drugs, or toxic substances during pregnancy
Malnourishment during pregnancy
Random malformation of the fetal brain
Small pelvis in the mother
Breech delivery
Brain damage after birth
A small proportion of cases happen because of damage after birth. This can happen because of an infection such as meningitis, a head injury, a drowning accident, or poisoning.
When damage occurs, it will do so soon after the birth. With age, the human brain becomes more resilient and able to withstand more damage.
Effects of Cerebral Palsy
The symptoms and effects of cerebral palsy vary, depending on the location and extent of the injury to the brain. Your child might have normal intelligence, or have learning difficulties. Your child might have mild difficulties with movement, or be unable to control their limbs. Despite the variations in symptoms, certain effects are common among people who have cerebral palsy.
Primary Physical Effects of Cerebral Palsy
Typical cerebral palsy symptoms include:
Abnormal muscle tone (muscles with too much or too little tone).
Muscles that pull unevenly on the joints.
Abnormal reflexes (the persistence of primitive reflexes that people normally outgrow during infancy).
Balance and movement problems.
The primary effects of cerebral palsy may improve with some treatments.
Secondary Physical Effects of Cerebral Palsy
As your child grows and develops, the primary effects of cerebral palsy can lead to secondary effects, including:
Inadequate muscle growth, causes shortening of muscles and tendons (called contractures).
Bone deformities.
Misalignment of the joints.
Excessive fatigue with movement and walking.
Pain.
Treatments can often slow or correct the secondary effects of cerebral palsy.
Other Physical Effects of Cerebral Palsy
The primary and secondary effects of cerebral palsy can lead your child to adopt “coping responses”—ways of moving that compensate for challenges. For example, abnormal muscle tone in the legs can result in stiff knees that make walking difficult. Your child might compensate for this challenge by swinging their legs in a circle rather than a straight line when walking.
These effects typically improve following treatment of primary and secondary effects, especially if patients undergo rehabilitation therapy as part of a treatment plan.
Possible Associated Effects
Depending on how much and where the brain is injured, a child who has cerebral palsy might experience additional health, thinking, and learning challenges like:
Breathing difficulties.
Depression, anxiety, and mental health disorders.
Feeding and swallowing disorders (like dysphagia).
Hearing loss and vision problems.
Learning disabilities or cognitive impairment.
Seizures and epilepsy.
Sensory issues.
Sleep disorders.
Speech and language difficulties.
Symptoms of Cerebral Palsy
www.rxharun.com
Signs and symptoms can vary greatly. Movement and coordination problems associated with cerebral palsy may include:
Variations in muscle tone, such as being either too stiff or too floppy
Stiff muscles and exaggerated reflexes (spasticity)
Stiff muscles with normal reflexes (rigidity)
Lack of muscle coordination (ataxia)
Tremors or involuntary movements
Slow, writhing movements (athetosis)
Delays in reaching motor skills milestones, such as pushing up on arms, sitting up alone, or crawling
Favoring one side of the body, such as reaching with only one hand or dragging a leg while crawling
Difficulty walking, such as walking on toes, a crouched gait, a scissors-like gait with knees crossing, a wide gait, or an asymmetrical gait
Excessive drooling or problems with swallowing
Difficulty with sucking or eating
Delays in speech development or difficulty speaking
Difficulty with precise motions, such as picking up a crayon or spoon
Seizures
The disability associated with cerebral palsy may be limited primarily to one limb or one side of the body, or it may affect the whole body. The brain disorder causing cerebral palsy doesn’t change with time, so the symptoms usually don’t worsen with age. However, muscle shortening and muscle rigidity may worsen if not treated aggressively.
Brain abnormalities associated with cerebral palsy also may contribute to other neurological problems. People with cerebral palsy may also have:
Difficulty with vision and hearing
Intellectual disabilities
Seizures
Abnormal touch or pain perceptions
Oral diseases
Mental health (psychiatric) conditions
Urinary incontinence
Treatment of Cerebral Palsy
Cerebral palsy can’t be cured – but treatment will often improve a child’s capabilities. Many children go on to enjoy near-normal adult lives if their disabilities are properly managed. In general, the earlier treatment begins, the better chance children have of overcoming developmental disabilities or learning new ways to accomplish the tasks that challenge them.
There is no standard therapy – that works for every individual with cerebral palsy. Once the diagnosis is made, and the type of CP is determined, a team of healthcare professionals will work with a child and his or her parents to identify specific impairments and needs, and then develop an appropriate plan to tackle the core disabilities that affect the child’s quality of life.
Occupational therapy – focuses on optimizing upper body function, improving posture, and making the most of a child’s mobility. Occupational therapists help individuals address new ways to meet everyday activities such as dressing, going to school, and participating in day-to-day activities.
Recreation therapy – encourages participation in art and cultural programs, sports, and other events that help an individual expand physical and cognitive skills and abilities. Parents of children who participate in recreational therapies usually notice an improvement in their child’s speech, self-esteem, and emotional well-being.
Speech and language therapy – can improve a child’s ability to speak, more clearly, help with swallowing disorders, and learn new ways to communicate—using sign language and/or special communication devices such as a computer with a voice synthesizer, or a special board covered with symbols of everyday objects and activities to which a child can point to indicate his or her wishes.
Treatments for problems with eating and drooling – are often necessary when children with CP have difficulty eating and drinking because they have little control over the muscles that move their mouth, jaw, and tongue. They are also at risk for breathing food or fluid into the lungs, as well as for malnutrition, recurrent lung infections, and progressive lung disease.
Therapies used to manage spasticity in cerebral palsy
Therapy
studies (patients studied)
randomized trials ( patients randomized)
Conclusions
Botulinum toxin type A in the treatment of lower limb spasticity
3 (52)
3 (52)
no strong controlled evidence was found to support or refute the use of Botulinum toxin type A for the treatment of leg spasticity (1)
Botulinum toxin type A for treatment of spastic equinus foot
Not provided
4 (183)
Botulinum toxin type A superior to a placebo for the improvement of gait(2)
Botulinum toxin A as an adjunct to treatment in the management of the upper limb in children with spastic cerebral palsy
2 (44)
2 (44)
one of the two randomized trials reported promising results in support of reduced muscle tone following Botulinum toxin A injections; the evidence is not sufficient to support or refute the use of this therapy as an adjunct to managing the upper limb in children with spastic cerebral palsy (3)
selective’ dorsal rhizotomy plus physiotherapy
3 (90)
3 (90)
selective’ dorsal rhizotomy (SDR) plus physiotherapy reduces spasticity in children with spastic diplegia and slightly improves gross motor function (4)
casting for equines
21 (473)
9 (238)
No randomized trials are available comparing protocols of casting in current use with no treatment; no strong and consistent evidence that combining casting and Botulinum toxin A is superior to using either intervention alone; no evidence that the order of these two treatments affects the outcome(5)
Therapies used to improve function in children with cerebral palsy
Therapy
studies (patients studied)
randomized trials (patients randomized)
Conclusions
Speech and language therapy to improve communication skills
11 (46)
1 (20)
the trend towards improved communication skills; evidence not sufficient to recommend a change in practice (1)
Constraint-induced movement therapy in the treatment of the upper limb in children with hemiplegic cerebral palsy
3 (94)
2 (49)
a significant benefit in a single trial; positive trend favoring constraint-induced movement therapy (CIMT) and Forced Use; “given the limited evidence, the use of CIMT, modified CIMT and Forced Use should be considered experimental in children with hemiplegic cerebral palsy.” (2)
Hyperbaric oxygen therapy
6 (449)
2 (137)
Hyperbaric oxygen therapy and pressurized room air improved function to a similar degree; a proportion of patients treated with these therapy experience seizures (3)
Pennington L, Goldbart J, Marshall J. Cochrane Collaboration. 2003.
Ade-Hall RA, Moore AP. Cochrane Collaboration. 2000. McDonagh MS, Morgan D, Carson S, Russman BS. Dev Med Child Neurol 2007; 49:942-947.
Drug Treatments
Nonoperative modalities, such as medication, splinting and bracing, and physical therapy, are commonly used as primary treatment or in conjunction with other forms of treatment such as surgery.[rx]–[rx]
Oral medications such as
Diazepam,
Baclofen
Tolperisone and Eperisone relax muscles to increase muscle tone
Phenobarbitone
Gabapentin/Pregabalin inhibits the pain receptor in the brain.
Mecobalamin /vitamin B12 regenerates the myelin sheet in the nervous system.
Steroids suppress brain inflammation.
Clonazepam drops to control salivation & proper sleep.
Tizanidine – is usually used as the first line of treatment to relax stiff, contracted, or overactive muscles. Some drugs have some risky side effects such as drowsiness, changes in blood pressure, and the risk of liver damage that require continuous monitoring. Oral medications are most appropriate for children who need only a mild reduction in muscle tone or who have widespread spasticity.
Botulinum toxin(BT-A) – injected locally, has become a standard treatment for overactive muscles in children with spastic movement disorders such as CP. BT-A relaxes contracted muscles by keeping nerve cells from over-activating muscle. The relaxing effect of a BT-A injection lasts approximately 3 months. Undesirable side effects are mild and short-lived, consisting of pain upon injection and occasionally mild flu-like symptoms. BT-A injections are most effective when followed by a stretching program including physical therapy and splinting. BT-A injections work best for children who have some control over their motor movements and have a limited number of muscles to treat, none of which is fixed or rigid.
Intrathecal baclofen- therapy uses an implantable pump to deliver baclofen, a muscle relaxant, into the fluid surrounding the spinal cord. Baclofen decreases the excitability of nerve cells in the spinal cord, which then reduces muscle spasticity throughout the body. The pump can be adjusted if muscle tone is worse at certain times of the day or night. The baclofen pump is most appropriate for individuals with chronic, severe stiffness or uncontrolled muscle movement throughout the body
Dantrolene – a peripheral-acting drug, acts at the level of skeletal muscle and selectively decreases abnormal muscle stretch reflexes and tone. Dantrolene is used less frequently than other medications because some patients taking it to develop profound weakness, and there is a risk of hepatotoxicity with its long-term use.
Common medications used to treat cerebral palsy
Each child with cerebral palsy is likely to have a unique combination of medications to treat their specific condition. Some medications are short-term, while others are long-term. Medications and dosages are often used in combination and will likely be adjusted over time.
Common classes of medications for children with cerebral palsy include:
Anticonvulsants
Antidepressants
Anti-inflammatories
Muscle relaxants
Benzodiazepines
Nerve blocks
Botox
Baclofen
Anticholinergics
Stool Softeners
Medications for spasticity
Spasticity is a condition where certain muscles contract continuously and involuntarily. This is the most common movement problem in children with cerebral palsy.
Spastic cerebral palsy causes spasms and stiff muscles. causes spasms and stiff muscles. This can be painful. Medications to control these symptoms may be given orally or through an injection. Some can be continuously infused through a small pump similarly to how Insulin can be given to diabetics.
Generalized spasticity is typically treated with muscle relaxants such as Baclofen or Botox and benzodiazepines such as Valium. Other medications can also be effective, and the healthcare team can help weigh the risks with the benefits
If spasticity is localized in a specific area, medication may be injected into those muscles. Botox is often used to reduce localized spasticity.
Common side effects from medications that reduce spasticity include:
Fatigue
Weakness
Loss of coordination
Dizziness
Headaches
Blurred vision
Nausea
There are also more serious short and long-term side effects and some medications are not recommended for children.
Medications for involuntary movement
Athetoid cerebral palsy (also known as dyskinetic cerebral palsy) is characterized by low muscle tone and involuntary movements. abnormal muscle tone and involuntary movements. Children with dyskinetic CP may be prescribed medications to keep uncontrollable movements to a minimum.
Anticholinergic drugs ease symptoms by blocking nerve impulses that cause uncontrollable movements. They may also help control drooling, a common symptom of dyskinetic cerebral palsy.
Common side effects include:
Incontinence
Dry mouth
Dizziness
Constipation
Medications for seizures
Injuries to the brain increase the likelihood of developing seizures. Therefore, it isn’t surprising that many children with cerebral palsy develop some form of epilepsy. A report by the Centers for Disease Control in 2008 found that 41 percent of children with CP across multiple states had co-occurring epilepsy. Several medications reduce the frequency of seizures.
Two common types of medications used to treat seizures are barbiturates and benzodiazepines. Both slow the activity of the brain and nervous system which helps prevent seizures. Phenobarbital is a common barbiturate medication given to newborns with seizure activity. Benzodiazepines that are often prescribed include Valium, Ativan, Dilantin, and Versed. These drugs are useful anticonvulsants, muscle relaxants, and anti-anxiety drugs.
Anticonvulsant medications, such as Keppra, are commonly used in children with CP to prevent seizure activity.
Some of the common side effects of these drugs include:
Dizziness
Weakness
Fatigue
Confusion
Hypotension
Get the help you need.
Find out how we can help you cover the cost of your child’s treatment.
Free case review
Secondary conditions treated with medications
Secondary conditions are common in children with cerebral palsy and other birth injuries because of abnormal muscle movement and brain activity. Some examples of co-occurring conditions are acid reflux, constipation or incontinence, respiratory issues, and difficulty with feeding. Additionally, the brain damage that causes CP may also cause separate issues, such as intellectual disorders that require medication.
Incontinence
The inability to control urinary muscles often leads to incontinence. Tofranil is an antidepressant that can also be used to contract the bladder and neck muscles and control incontinence. DDAVP (desmopressin acetate) mimics natural hormones to decrease urine production and can be used as a nasal spray.
Acid reflux
A secondary issue caused by a lack of muscle control is gastroesophageal reflux. In children with CP, the muscle that prevents stomach acid from traveling up the esophagus may not be strong enough to prevent acid reflux. Over-the-counter medications that decrease acid production in the stomach, such as Zantac, are often beneficial.
Behavioral disorders
Some children with cerebral palsy develop behavioral or intellectual disorders. Attention deficit hyperactivity disorder (ADHD) and autism are common in children with CP. Adderall and Ritalin are some of the most common medications used to treat ADHD. Antipsychotic medications, such as Risperidone, are used to help with Autism symptoms.
Constipation
Lactulose is a synthetic sugar used to treat constipation. MiraLax is often used to treat children with constipation. It works by drawing water into the bowels to help soften stool and move it through the GI tract. This is considered to have low side effects.
Increased oral secretions
Children with CP often have limited or no motor control leading to excessive drooling. Anticholinergic medications, such as Rubino, are effective in controlling the increased oral secretions.
Is medication necessary?
Many parents are understandably concerned about placing their children on medications. Fear of side effects and dependence on these medications often lead parents to explore alternatives.
Activities such as yoga, chiropractic care, music, aquatic therapy, acupuncture, and occupational, and physical therapy can be effective in treating the symptoms related to CP and are often used in conjunction with medications.
Doctors and members of the care team can help decide what is best for your loved one. Please consult your child’s doctor before changing or discontinuing any medications. Doctors strive to tailor medications to each child’s specific needs. Discussing your goals and quality of life expectations with your child’s care providers can help your family find the best strategies to balance CP and its challenges.
Surgery
Surgery to cut nerves – Selective dorsal rhizotomy (SDR) is a surgical procedure recommended for cases of severe spasticity when all of the more conservative treatments – physical therapy, oral medications, and intrathecal baclofen — have failed to reduce spasticity or chronic pain. A surgeon locates and selectively severs overactivated nerves at the base of the spinal column. SDR is most commonly used to relax muscles and decrease chronic pain in one or both of the lower or upper limbs. It is also sometimes used to correct an overactive bladder. Potential side effects include sensory loss, numbness, or uncomfortable sensations in limb areas once supplied by the severed nerve.
Orthopedic surgery
Orthopedic surgery is often recommended when spasticity and stiffness are severe enough to make walking and moving about difficult or painful. For many people with CP, improving the appearance of how they walk – their gait – is also important. Surgeons can lengthen muscles and tendons that are proportionately too short, which can improve mobility and lessen pain. Tendon surgery may help the symptoms of some children with CP but could also have negative long-term consequences. Orthopedic surgeries may be staggered at times appropriate to a child’s age and level of motor development. Surgery can also correct or greatly improve spinal deformities in people with CP. Surgery may not be indicated for all gait abnormalities and the surgeon may request a quantitative gait analysis before surgery.
The 6 main types of orthopedic procedures are:
Muscle lengthening – Surgical lengthening of the muscles used to relieve tightness in the hands and fingers. Lengthening the arm muscles can help children grasp objects more easily and improve fine motor skills.
Tendon lengthening – Lengthening tendons can reduce painful contractures, which is a permanent tightening of the tendons or muscles. This surgery is often used to improve a child’s ability to walk and sit upright.
Tendon transfer – Tendon transfers typically involve the cutting and replacement of a tendon. The goal of tendon transfers is to ensure that the muscles in the body are properly aligned. This surgery also helps reduce any pain or walking problems that children with CP may be experiencing, as well as improves the extension and flexibility of the wrists.
Tenotomy/myotomy – Tenotomy describes the cutting of the tendon, whereas myotomy involves cutting the muscle. This procedure is used to improve muscle function, increase control of the upper limbs and enhance the ability to grasp objects with hands and feet.
Osteotomy – This procedure is used to realign joints for better posture and mobility. It involves repositioning bones at angles more conducive to healthy alignments and is commonly used to correct hip dislocations in children with CP.
Arthrodesis – In severe cases of spasticity, when splints and casts aren’t enough, arthrodesis may be used to permanently fuse bones. Fusing the bones in the ankle and foot can make it easier for a child to walk.
The type of orthopedic surgery that would be best for your child depends mostly on whether they are considered to be ambulatory or not. An ambulatory child can walk around independently or with the use of mobility aids such as crutches or walkers. A nonambulatory child is unable to walk or requires the use of a wheelchair to move about.
AmbulatoryAmbulatory children with cerebral palsy may tend to step mostly on their toes, cross their hips while walking or bend their knees when taking strides. These issues can be caused by tight muscles, weakness, or misalignment of the joints or bones.
The purpose of surgery for ambulatory children is to improve their ability to walk, which is essential to improving self-reliance. For example, a child who “toe-walks” may have their stride corrected with a tenotomy or tendon lengthening procedure. Orthopedic surgery can also correct issues caused by poor alignment of the hips or knees.
Non-ambulatoryNon-ambulatory children are unable to walk, which is why the goal of orthopedic surgery is more centered around increasing comfort and avoiding any further mobility complications.
Orthopedic surgery is used to stop certain complications from getting worse. Surgeries correcting spinal curvature, hip dislocations, and contractures alleviate pain and promote a comfortable, well-aligned sitting position. Osteotomy may be used to fuse bones in the spine to correct severe scoliosis.
The benefits of orthopedic surgery aren’t immediate. Children often require physical therapy to ensure a successful recovery and to keep muscles strong and flexible.
Selective dorsal rhizotomySelective dorsal rhizotomy (SDR) is an aggressive procedure that helps reduce pain and spasticity. SDR is typically recommended in severe cases of spasticity when other treatments have failed to make an impact. Children with spasticity in the legs (spastic diplegia) tend to benefit more than children with spasticity in other locations (quadriplegia, hemiplegia).
Selective dorsal rhizotomy gets to the root of spasticity issues by cutting the nerves in the spinal column responsible for muscle stiffness. This procedure requires navigating the complex network of nerves to pinpoint which nerves are causing movement issues. SDR can be used to relax muscles in the upper and lower limbs.
Selective dorsal rhizotomy improves:
Walking
Sitting
Standing
Balance
Deformities in tendons, muscles, feet, and hips
Voluntary movement
Recovery from selective dorsal rhizotomy requires intensive physical therapy to relearn muscle control and movement.
Other conditions
Cerebral palsy affects every child differently, and most children who have it experience secondary conditions, such as hearing loss or acid reflux. These secondary conditions can be a result of limited movement caused by cerebral palsy, or they may be a direct result of the brain injury experienced at birth.
Assistive devices
Assistive devices such devices as computers, computer software, voice synthesizers, and picture books can greatly help some individuals with CP improve their communication skills. Other devices around the home or workplace make it easier for people with CP to adapt to activities of daily living.
Orthotic devices help to compensate for muscle imbalance and increase independent mobility. Braces and splints use external force to correct muscle abnormalities and improve functions such as sitting or walking. Other orthotics help stretch muscles or the position of a joint. Braces, wedges, special chairs, and other devices can help people sit more comfortably and make it easier to perform daily functions. Wheelchairs, rolling walkers, and powered scooters can help individuals who are not independently mobile. Vision aids include glasses, magnifiers, large-print books, and computer typefaces. Some individuals with CP may need surgery to correct vision problems. Hearing aids and telephone amplifiers may help people hear more clearly.
Complementary and Alternative Therapies
Many children and adolescents with CP use some form of complementary or alternative medicine. Controlled clinical trials involving some of the therapies have been inconclusive or showed no benefit and the therapies have not been accepted in mainstream clinical practice.
Although there are anecdotal reports of some benefits in some children with CP, these therapies have not been approved by the U.S. Food and Drug Administration for the treatment of CP.
Such therapies include hyperbaric oxygen therapy, special clothing worn during resistance exercise training, certain forms of electrical stimulation, assisting children in completing certain motions several times a day, and specialized learning strategies. Also, dietary supplements, including herbal products, may interact with other products or medications a child with CP may be taking or have unwanted side effects on their own. Families of children with CP should discuss all therapies with their doctor.
Stem cell therapy – is being investigated as a treatment for cerebral palsy, but research is in the early stages and large-scale clinical trials are needed to learn if stem cell therapy is safe and effective in humans. Stem cells are capable of becoming other cell types in the body. Scientists are hopeful that stem cells may be able to repair damaged nerves and brain tissues. Studies in the U.S. are examining the safety and tolerability of umbilical cord blood stem cell infusion in children with CP.
How surgery can help
Surgery is one of the many options available to help children with cerebral palsy improve mobility, and posture and ensure healthy growth. Most doctors recommend physical therapy and medication before surgery.
Surgery can correct or improve movement and alignment in the legs, ankles, feet, hips, wrists, and arms. These operations are performed on the muscles, tendons, bones, and nerves.
As is the goal with all treatment of cerebral palsy, surgery aims to give children the greatest chance of living as independently as possible. Movement problems caused by cerebral palsy can improve over time, but they also carry the risk of getting worse.
The main purpose of surgery is to make a child’s cerebral palsy more manageable and prevent future complications.
Many children with cerebral palsy have a hearing impairment. Those with severe hearing loss may benefit from cochlear implants—a surgically implanted hearing devices. Congenital hearing impairment (loss of hearing present at birth) can be caused by the same factors that cause cerebral palsy, such as oxygen deprivation during birth. As many as 15 percent of children with CP have a hearing impairment.
Gastrostomy
Children with low muscle tone often have issues with feeding. Their lack of muscle control can make it hard for them to swallow and chew. They may also have severe acid reflux or experience aspiration (food and drink entering the lungs) as a result of low muscle tone. Children can avoid these complications by having a feeding tube surgically implanted. For children with severe cerebral palsy, this may be the only way they can stay healthy. It also makes feeding time less demanding for parents. For children with less severe diagnoses, speech therapists can help with chewing and swallowing.
Hydrocephalus
This is a rare condition that can require surgical treatment. Hydrocephalus is a complication involving the buildup of cerebrospinal fluid in the skull, causing an abnormal increase in the size of the head. Untreated, this condition can be fatal. Treatment can include the implantation of valves to drain off excess fluid. Few children with cerebral palsy have hydrocephalus.
When is surgery appropriate?
Every surgery has its risks. Collaboration between parents and doctors can help families weigh the possible benefits with the risks of surgery. It takes careful consideration to determine when surgery is appropriate because every child is different.
Doctors have differing opinions about the best time in a child’s life to suggest surgery. Some doctors think surgery offers the greatest benefit when children are young; others think it’s best to wait until children are older, recommending physical therapy and medication in the meantime. Generally, children with cerebral palsy are treated between the ages of 3 and 10, but the exact age depends on the individual.
Risk factors
Several factors are associated with an increased risk of cerebral palsy.
Maternal health – Certain infections or health problems during pregnancy can significantly increase the cerebral palsy risk to the baby. Infections of particular concern include:
German measles (rubella) – Rubella is a viral infection that can cause serious birth defects. It can be prevented with a vaccine.
Chickenpox (varicella) – Chickenpox is a contagious viral infection that causes itching and rashes, and it can cause pregnancy complications. It too can be prevented with a vaccine.
Cytomegalovirus – Cytomegalovirus is a common virus that causes flu-like symptoms and may lead to birth defects if a mother experiences her first active infection during pregnancy.
Herpes – Herpes infection can be passed from mother to child during pregnancy, affecting the womb and placenta. Inflammation triggered by infection may then damage the unborn baby’s developing nervous system.
Toxoplasmosis – Toxoplasmosis is an infection caused by a parasite found in contaminated food, soil, and the feces of infected cats.
Syphilis – Syphilis is a sexually transmitted bacterial infection.
Exposure to toxins – Exposure to toxins, such as methyl mercury, can increase the risk of birth defects.
Zika virus infection – Infants for whom maternal Zika infection causes microcephaly can develop cerebral palsy.
Other conditions. Other conditions may increase the risk of cerebral palsy, such as thyroid problems, intellectual disabilities, or seizures.
Infant illness
Illnesses in a newborn baby that can greatly increase the risk of cerebral palsy include:
Bacterial meningitis –This bacterial infection causes inflammation in the membranes surrounding the brain and spinal cord.
Viral encephalitis – This viral infection similarly causes inflammation in the membranes surrounding the brain and spinal cord.
Severe or untreated jaundice – Jaundice appears as a yellowing of the skin. The condition occurs when certain byproducts of “used” blood cells aren’t filtered from the bloodstream.
Other factors of pregnancy and birth
While the potential contribution from each is limited, additional pregnancy or birth factors associated with increased cerebral palsy risk include:
Breech births – Babies with cerebral palsy are more likely to be in a feet-first position (breech presentation) at the beginning of labor rather than headfirst.
Complicated labor and delivery – Babies who exhibit vascular or respiratory problems during labor and delivery may have existing brain damage or abnormalities.
Low birth weight – Babies who weigh less than 5.5 pounds (2.5 kilograms) are at higher risk of developing cerebral palsy. This risk increases as birth weight drop.
Multiple babies – Cerebral palsy risk increases with the number of babies sharing the uterus. If one or more of the babies die, the chance that the survivors may have cerebral palsy increases.
Premature birth – A normal pregnancy lasts 40 weeks. Babies born fewer than 37 weeks into pregnancy are at higher risk of cerebral palsy. The earlier a baby is born, the greater the cerebral palsy risk.
Rh blood type incompatibility between mother and child – If a mother’s Rh blood type doesn’t match her baby’s, her immune system may not tolerate the developing baby’s blood type and her body may begin to produce antibodies to attack and kill her baby’s blood cells, which can cause brain damage.
Complications
Muscle weakness, muscle spasticity, and coordination problems can contribute to several complications either during childhood or later during adulthood, including:
Contracture – Contracture is muscle tissue shortening due to severe muscle tightening (spasticity). Contracture can inhibit bone growth, cause bones to bend, and result in joint deformities, dislocation, or partial dislocation.
Malnutrition – Swallowing or feeding problems can make it difficult for someone who has cerebral palsy, particularly an infant, to get enough nutrition. This may cause impaired growth and weaker bones. Some children may need a feeding tube for adequate nutrition.
Mental health conditions – People with cerebral palsy may have mental health (psychiatric) conditions, such as depression. Social isolation and the challenges of coping with disabilities can contribute to depression.
Lung disease – People with cerebral palsy may develop lung disease and breathing disorders.
Neurological conditions – People with cerebral palsy may be more likely to develop movement disorders or worsened neurological symptoms over time.
Osteoarthritis – Pressure on joints or abnormal alignment of joints from muscle spasticity may lead to the early onset of painful degenerative bone disease (osteoarthritis).
Osteopenia – Fractures due to low bone density (osteopenia) can stem from several common factors such as lack of mobility, nutritional shortcomings, and antiepileptic drug use.
Eye muscle imbalance – This can affect visual fixation and tracking; an eye specialist should evaluate suspected imbalances.
Low birth weight and premature birth – Premature babies (born less than 37 weeks into pregnancy) and babies weighing less than 5 ½ pounds at birth have a much higher risk of developing cerebral palsy than full-term, heavier-weight babies. Tiny babies born at very early gestational ages are especially at risk.
Multiple births – Twins, triplets, and other multiple births — even those born at term — are linked to an increased risk of cerebral palsy. The death of a baby’s twin or triplet further increases the risk.
Infections during pregnancy – Infections such as toxoplasmosis, rubella (German measles), cytomegalovirus, and herpes, can infect the womb and placenta. Inflammation triggered by infection may then go on to damage the developing nervous system in an unborn baby. Maternal fever during pregnancy or delivery can also set off this kind of inflammatory response.
Blood type incompatibility between mother and child –Rh incompatibility is a condition that develops when a mother’s Rh blood type (either positive or negative) is different from the blood type of her baby. The mother’s system doesn’t tolerate the baby’s different blood type and her body will begin to make antibodies that will attack and kill her baby’s blood cells, which can cause brain damage.
Exposure to toxic substances – Mothers who have been exposed to toxic substances during pregnancy, such as methyl mercury, are at a heightened risk of having a baby with cerebral palsy.
Mothers with thyroid abnormalities, intellectual disability, excess protein in the urine, or seizures – Mothers with any of these conditions are slightly more likely to have a child with CP. There are also medical conditions during labor and delivery, and immediately after delivery that act as warning signs for an increased risk of CP. However, most of these children will not develop CP. Warning signs include:
Breech presentation – Babies with cerebral palsy are more likely to be in a breech position (feet first) instead of head first at the beginning of labor. Babies who are unusually floppy as fetuses are more likely to be born in the breech position.
Complicated labor and delivery – A baby who has vascular or respiratory problems during labor and delivery may already have suffered brain damage or abnormalities.
Small for gestational age – Babies born smaller than normal for their gestational age are at risk for cerebral palsy because of factors that kept them from growing naturally in the womb.
Low Apgar score –The Apgar score is a numbered rating that reflects a newborn’s physical health. Doctors periodically score a baby’s heart rate, breathing, muscle tone, reflexes, and skin color during the first minutes after birth. A low score 10-20 minutes after delivery is often considered an important sign of potential problems such as CP.
Jaundice – More than 50 percent of newborns develop jaundice (yellowing of the skin or whites of the eyes) after birth when bilirubin, a substance normally found in bile, builds up faster than their livers can break it down and pass it from the body. Severe, untreated jaundice can kill brain cells and can cause deafness and CP.
Are there treatments for other conditions associated with cerebral palsy?
Epilepsy
Many children with intellectual disabilities and CP also have epilepsy. In general, drugs are prescribed based on the type of seizures an individual experiences, since no one drug controls all types. Some individuals may need a combination of two or more drugs to achieve good seizure control.
Incontinence
Medical treatments for incontinence include special exercises, biofeedback, prescription drugs, surgery, or surgically implanted devices to replace or aid muscles.
Osteopenia
Children with CP who are unable to walk risk developing poor bone density (osteopenia), which makes them more likely to break bones. In a study of older Americans funded by the National Institutes of Health (NIH), a family of drugs called bisphosphonates, which has been approved by the FDA to treat mineral loss in elderly patients, also appeared to increase bone mineral density Doctors may choose to selectively prescribe the drug off-label to children to prevent osteopenia.
Pain
Pain can be a problem for people with CP due to spastic muscles and the stress and strain on parts of the body that are compensating for muscle abnormalities. Some individuals may also have frequent and irregular muscle spasms that can’t be predicted or medicated in advance.
Diazepam can reduce the pain associated with muscle spasms and gabapentin has been used successfully to decrease the severity and frequency of painful spasms. Botulinum toxin injections have also been shown to decrease spasticity and pain.
Intrathecal baclofen has shown good results in reducing pain. Some children and adults have been able to decrease pain by using noninvasive and drug-free interventions such as distraction, relaxation training, biofeedback, and therapeutic massage.
Premature aging
The majority of individuals with CP will experience some form of premature aging by the time they reach their 40s because of the extra stress and strain the disease puts upon their bodies.
The developmental delays that often accompany CP keep some organ systems from developing to their full capacity and level of performance. As a consequence, organ systems such as the cardiovascular system (the heart, veins, and arteries) and pulmonary system (lungs) have to work harder and they age prematurely.
Functional issues at work
The day-to-day challenges of the workplace are likely to increase as an employed individual with CP reaches middle age. Some individuals will be able to continue working with accommodations such as an adjusted work schedule, assistive equipment, or frequent rest periods.
Depression
Mental health issues can also be of concern as someone with cerebral palsy grows older. The rate of depression is three to four times higher in people with disabilities such as cerebral palsy.
It appears to be related not so much to the severity of their disabilities, but to how well they cope with them. The amount of emotional support someone has, how successful they are at coping with disappointment and stress, and whether or not they have an optimistic outlook about the future all have a significant impact on mental health.
Post-impairment syndrome
This syndrome is marked by a combination of pain, fatigue, and weakness due to muscle abnormalities, bone deformities, overuse syndromes (sometimes also called repetitive motion injuries), and arthritis. Fatigue is often a challenge, since individuals with CP may use up to three to five times the amount of energy that able-bodied people use when they walk and move about.
Osteoarthritis and degenerative arthritis
Musculoskeletal abnormalities that may not produce discomfort during childhood can cause pain in adulthood. For example, the abnormal relationships between joint surfaces and excessive joint compression can lead to the early development of painful osteoarthritis and degenerative arthritis.
Individuals with CP also may have limited strength and restricted patterns of movement, which puts them at risk for overuse syndromes and nerve entrapments.
Other medical conditions
Adults have higher than normal rates of other medical conditions secondary to their cerebral palsy, such as hypertension, incontinence, bladder dysfunction, and swallowing difficulties.
Scoliosis is likely to progress after puberty when bones have matured into their final shape and size. People with CP also have a higher incidence of bone fractures, occurring most frequently during physical therapy sessions.
Genetic defects are sometimes responsible for brain malformations and abnormalities that cause cerebral palsy. Scientists are searching for the genes responsible for these abnormalities by collecting DNA samples from people with cerebral palsy and their families and using genetic screening techniques to discover linkages between individual genes and specific types of abnormality – primarily those associated with the process in the developing brain in which neurons migrate from where they are born to where they settle into neural circuits (called neural migration).
Scientists are scrutinizing events in newborn babies’ brains, such as bleeding, epileptic seizures, and breathing and circulation problems, which can cause the abnormal release of chemicals that triggers the kind of damage that causes cerebral palsy. For example, research has shown that bleeding in the brain unleashes dangerously high amounts of glutamate, a chemical that helps neurons communicate. However, too much glutamate overexcites and kills neurons. By learning how brain chemicals that are normally helpful become dangerously toxic, scientists will have opportunities to develop new drugs to block their harmful effects.
Researchers are using imaging techniques and neurobehavioral tests to predict those preterm infants who will develop cerebral palsy. If these screening techniques are successful, doctors will be able to identify infants at risk for cerebral palsy before they are born.
Periventricular white matter damage—the most common cause of CP—is characterized by the death of the white matter around the fluid-filled ventricles in the brain. The periventricular area contains nerve fibers that carry messages from the brain to the body’s muscles. NINDS-sponsored researchers are hoping to develop preventative strategies for white matter damage. For example, researchers are examining the role brain chemicals play in white matter development in the brain.
NIH-funded scientists continue to look at new therapies and novel ways to use existing options to treat individuals with CP, including:
Constraint-induced therapy (CIT) – is a promising therapy for CP. CIT typically involves restraining the stronger limb (such as the “good” arm in a person who has been affected by a stroke on one side of the body) in a cast and forcing the weaker arm to perform intensive activities every day for weeks. A clinical study sponsored by the NICHD is examining the use of different dosage levels of daily training using either full-time cast immobilization vs. part-time splint restraint in improving upper body extremity skills in children with weakness on both sides of their body. Study findings will establish evidence-based practice standards to improve lifelong neuromotor capacity in individuals with CP.
Functional electrical stimulation (FES)—the therapeutic use of low-level electrical current to stimulate muscle movement and restore useful movements such as standing or stepping—is an effective way to target and strengthen spastic muscles. Researchers are evaluating how FES-assisted stationary cycling can improve physical conditioning and general lower extremity muscle strength in adolescents.
Robotic therapy – which applies controlled force to the leg during the swing phase of gait is may improve the efficacy of body weight-supported treadmill training in children with CP. The results from this NICHD study will lead to an innovative clinical therapy aimed at improving locomotor function in children with CP.
Botulinum toxin (Botox) – injected locally, has become a standard treatment in children with spastic movement disorders such as CP. Recent animal studies suggest Botox degrades bone but there are no studies of its skeletal consequences in humans. Other research shows a low-intensity vibration treatment can improve bone structure in the lower extremity leg bones of children with CP. In a novel clinical study being conducted by NICHD, researchers are determining the effect of Botox treatment in conjunction with a daily vibration treatment on bone mass and bone structure in children with spastic CP.
Systemic hypothermia—the controlled medical cooling of the body’s core temperature—appears to protect the brain and decrease the rate of death and disability from certain disorders and brain injuries. Previous studies have shown that hypothermia is effective in treating neurologic symptoms in term or late preterm babies less than the one-month-old that is attributed to hypoxic-ischemia (HIE, brain injury due to a severe decrease in the oxygen supply to the body), which can cause quadriplegic CP, with or without movement disorder. To determine the most effective cooling strategies, NICHD-funded researchers are studying different cooling treatments to improve the chance of survival and neurodevelopment outcomes 18-22 months post-treatment in infants with neurologic symptoms attributed to HIE. Other researchers are examining if combined therapy using hypothermia and recombinant erythropoietin (a hormone that promotes the growth of new red blood cells and increases oxygen levels in the blood) is more effective than either therapy alone in treating neurodevelopmental handicaps in an animal model involving a lack of oxygen before, during, or just after birth.
Physical Therapy
What is physical therapy?
Physical therapy (PT) is a branch of rehabilitative health that is considered one of the most important aspects of treating children with Cerebral Palsy. Those with Cerebral Palsy experience mobility, function, posture, and balance challenges of varying degrees, and physical therapy – which focuses on basic mobility such as standing, walking, climbing stairs, and reaching or operating a wheelchair – is a key element in the multidisciplinary approach to increasing a child’s mobility.
Physical therapy is the rehabilitation of physical impairments by training and strengthening a patient’s large muscles – those in the arms, legs, and abdomen. The goal of physical therapy is to maximize functional control of the body or increase gross motor function.
The goal of physical therapy is to help individuals:
develop coordination
build strength
improve balance
maintain flexibility
optimize physical functioning levels
maximize independence
Trained and licensed physical therapists identify mobility issues and determine the unique physical abilities and limitations of children, taking into account their age and cognitive functioning, after a diagnosis of Cerebral Palsy is made by a physician.
The therapist will then develop a course of treatment that will include exercises, stretches, and possibly assistive and adaptive equipment designed to achieve mobility. The treatment may also employ the use of passive modalities involving hot and cold packs, ultrasound technology, or other means in which the child does not take an active role.
All treatment is designed to meet a child’s individual needs in a way that emphasizes physical fitness and minimizes injuries and pain
Therapy aids overall treatment goals such as:
Overcoming physical limitations
Expanding the range of joint motion
Building and maintaining muscle tone
Increasing recreational capabilities
Identifying alternate ways to perform everyday tasks
Fostering independence
Decreasing the likelihood of contractures, bone deformity
Educating children and parents about adaptive equipment
Providing sensory stimulation
Increasing fitness
Increasing flexibility
Improving posture
Improving gait
Minimizing pain and discomfort
Who benefits from physical therapy?
A child, and his or her parents or caregivers, benefit tremendously from physical therapy because it helps the child overcome physical limitations by increasing mobility, and identifying alternate methods of completing tasks.
The individual with Cerebral Palsy benefits
This is of benefit to the child because it makes possible something unaffected individuals take for granted: the ability to move from place to place and interact with other children or adults by playing or performing tasks. Therapy also increases overall health by strengthening the body in a way that makes functioning not only possible but pain and stress-free.
This is achieved not only by developing strength and flexibility in the body but also by using adaptive techniques – or equipment that can be operated by the child – that will allow the patient an alternate path to perform tasks, able-bodied children, of their age perform.
Depending on the nature of a child’s Cerebral Palsy, a child can live a near-normal life; persons with the condition have attended college, participated in sports and activities, excelled in their careers, and have married.
Physical therapy empowers the child physically and emotionally and sets the stage for entering adulthood as an independent individual.
Parents and caregivers benefit
Parents and caregivers benefit because as a patient progresses, raising a child with Cerebral Palsy becomes less labor-intensive. Parents and caregivers are often overwhelmed and under an extreme level of stress.
They have several responsibilities, including assisting their child with many physical tasks, providing love and emotional support, making sure the child is receiving adequate care in a medical setting, and education at school. The more physical challenges a child can overcome or adapt to, the less hands-on assistance is required of the parents.
Additionally, a successful physical therapy program allows a parent to see their child healthily interacting with others, building relationships, using their body to the best of their ability, and potentially, living independently.
What are the benefits of physical therapy?
The benefit of physical therapy, for any patient that is experiencing physical limitations, is regaining – or developing – physical mobility.
By developing a comprehensive plan of treatment, a physical therapist can address limitations in a child’s mobility – and specifically address them. This is achieved through employing exercises that increase physical function and using adaptive equipment such as wheelchairs, walkers, canes, and orthotics to improve performance.
As a child’s physical abilities improve, the therapist can modify the equipment, or the overall course of therapy, to further advance a child’s treatment.
The largest benefit of therapy to the child with Cerebral Palsy is in the treatment of problematic conditions when they occur, including:
Muscle atrophy or tightening
Loss in joint range of motion
Muscle spasticity
Pain in muscles and joints
Joint inflammation
Contractures (muscle rigidity)
The therapists focus on achieving optimal results and minimizing unforeseen complications.
How is physical therapy performed?
Physical therapy is carried out by licensed physical therapists and physical therapy assistants, often by using means such as:
soft tissue mobilization (kneading of the muscles)
joint mobilization
specialized exercises
stretching
endurance exercises designed to meet therapeutic goals
Physical therapy is hands-on: a therapist, or an assistant, will guide the child through exercises.
Exercises often include the use of equipment, such as:
Weights
Exercise machines
Bands
Rollers
Balance balls
Heat and cold packs
Ultrasound technology
At some centers, sports or recreation like swimming, dancing, and playing games such as throwing and catching a ball, may be used to help children develop muscles, balance, coordination, and range of motion.
Swimming, because the child is almost entirely submerged in the water, will give children an opportunity to do exercises they cannot do otherwise; moving against the water, kicking and other beneficial exercises can be accomplished in a pool, sometimes in braces. These methods can provide children with an opportunity to play and have fun.
Adaptive equipment including braces, splints, walkers, orthotics, wheelchairs, and even computers will be used in therapy; therapists will modify the equipment as needed. The therapist will also play an instructive role in this regard for children and parents, teaching them how to use the equipment.
Where does physical therapy occur?
Physical therapy takes place in several settings, including outpatient medical offices or clinics, inpatient rehabilitation centers, specialized physical therapy centers, skilled nursing centers, hospitals, special education classrooms, and in the home.
The number of physical therapy settings is dependent on several factors; the most important of these is the prescribed treatment of the child. Additional considerations include what adaptive equipment is used in treatment, as well as the ability of a caregiver to provide additional therapy at home. Insurance coverage can also dictate how often a child attends therapy in a clinical setting.
In many cases, a physical therapist will prescribe exercises to be completed at home. The physical therapist or an assistant will train the individual with Cerebral Palsy, the parent or caregiver, and the primary caregivers on how to properly perform exercises at home.
What happens during physical therapy?
There is no therapeutic template for Cerebral Palsy since there are many forms of Cerebral Palsy that affect each individual differently.
All physical therapy begins with a diagnosis – the child’s primary doctor will then refer the child to a physical therapist while providing specific treatment goals to accomplish.
At the start of physical therapy, a comprehensive medical history of the child will be obtained. Additionally, the therapist will conduct a series of tests, observations, and measurements to assess the child’s body mechanics and function.
The examination may assess:
Gait
Range of joint motion
Physical strength
Flexibility
Balance
Endurance
Joint integrity
Posture
Neuromotor development
Sensory integration
Cognitive functioning
Reflexes
Breathing, respiration
The therapist then prepares a patient-centered plan of care that takes into account the child’s condition, and the child’s overall environment.
The physical therapist will also determine what orthotic equipment, adaptive equipment, or assistive technologies may be needed to help a child.
Orthotic equipment can include braces that stabilize the ankles, knees, legs, torso, upper arms, lower arms, elbows, or hands. Adaptive equipment includes strollers, nets, walkers, and wheelchairs. The therapist will teach the child – and his or her caregivers – how to operate the equipment, and will make modifications to accommodate the child’s condition.
Once the child’s plan of treatment is determined, therapists will set goals for a child’s progress, and work with the child to meet those benchmarks. This typically means the therapist and his or her assistants manipulate a child’s body while completing stretches, strength exercises, or games with specific movements or purposes.
Often therapy includes instructions for exercises, stretches, posturing and balance to be performed outside the therapy sessions; at home, school, or at work.
Who provides physical therapy?
Physical therapy is performed by licensed, accredited physical therapists, or physiotherapists. These professionals are often assisted by physical therapy assistants.
Practicing physical therapists may be doctors, some having earned a master’s degree in physical therapy or kinesiology.
The coursework a budding physical therapist must complete is extensive and includes:
biology
physics
chemistry
anatomy
physiology
kinesiology
human growth and development
examination
therapeutic practices
Physical therapy assistants – who worked under the supervision of a physical therapist –typically complete bachelor’s or associate degree programs focusing on the same topics as the physical therapist.
All states require licensure via state board examination to practice, though the requirements to take the exam vary from state to state. Most states require the therapist to complete the National Physical Therapy Examination; however, others administer their examination.
What is the difference between physical therapy and physiotherapy?
The job of the physical therapist and the physiotherapist is the same – to help a child develop muscular coordination, strength, flexibility, and balance to support their mobility.
Even though the two terms have been used interchangeably, there are some differences between the two professions. A physical therapist is trained to work in private physician practices, specialized centers, or clinics. Physiotherapists are found more often in hospitals.
There is also a slight difference in the approach to therapy; a physical therapist may concentrate solely on physical activities, while a physiotherapist may use ultrasounds or other electronic means to achieve goals.
Though there used to be several differences in training, most experts agree that the requirements to work as a physical therapist or a physiotherapist are very similar.
Is there any risk or special consideration for physical therapy?
Although physical therapists and their assistants are trained to minimize unforeseen circumstances while carrying out treatment plans with patients, there is some risk associated with therapy. Physical therapy is meant to be restorative – a therapist more often than not will not overwork a patient. However, this can occur.
If physical therapy is taken too far in a given session, this can cause injury or unnecessary pain, which is not the goal of therapy.
The key to minimizing risks and maximizing results is open communication between the child, his or her caregivers, and physical therapists. Identify where your child’s physical and psychological limits are. Talk to your child regularly to discover difficult areas of therapy. Don’t be afraid to mention your concerns to the therapist.
Adduction deformities
Adduction is the most common deformity of the hip in children with cerebral palsy. Adduction contractures can cause various difficulties, including scissoring of the legs, hip subluxation, and in severely affected children, difficulty with perineal hygiene.
For mild contractures, an adductor tenotomy usually is sufficient; more severe contractures often require the additional release of the gracilis and the anterior half of the adductor Brevis. Neurectomy of the anterior branch of the obturator nerve should be avoided to prevent iatrogenic hip abduction contracture.[rx–RX
Flexion deformities
Excessive hip flexion brings the center of gravity anteriorly and is compensated for by increased lumbar lordosis, knee flexion, and ankle dorsiflexion. It is important to determine whether the increased hip flexion is the primary deformity or is compensatory to other deformities around the lower extremities, such as knee or ankle contractures. If an unrecognized knee flexion contracture is present, hip flexor release can weaken the hip further and increase hip flexion.
Hip flexion contractures of 15–30° are usually treated with psoas lengthening through an intramuscular recession over the pelvic brim. Contractures of more than 30° may require more extensive releases of the rectus femoris, sartorius, and tensor fasciae late and the anterior fibers of the gluteus minimus and medius, in addition to the iliopsoas.
Subluxation and dislocation
Hip subluxation and dislocation occur in 7% of ambulators and 60% of dependent sitters. The cause of this progressive deformity of the hip is multifactorial and includes muscle imbalance, retained primitive reflexes, abnormal positioning, pelvic obliquity, acetabular dysplasia, excessive femoral anteversion, and increased neck-shaft angle, and osteopenia.
Hip subluxation in patients with cerebral palsy can be difficult to detect clinically because of the presence of abnormal muscle forces and contractures, and because early hip subluxation typically is painless. Routine clinical and radiographic examinations should be done every 6 months, especially in rapidly growing children and patients with spastic quadriplegia.
Clinically, hips with flexion contractures of more than 20° and abduction of less than 30° are at increased risk of progressive subluxation. Radiographically, a hip at risk has an increased neck-shaft angle and increased femoral anteversion. When a hip at risk is identified, a program of aggressive physical therapy and abduction splinting is started. If further progression continues, operative treatment consisting of the soft-tissue release of contracted tendons is indicated.
Operative correction of femoral valgus and anteversion and acetabular dysplasia is sometimes necessary at this stage. The treatment of an established dislocation is more controversial. A patient with a long-standing dislocation is not a good candidate for a relocation procedure because of the deformities of the proximal femur and acetabulum.
Resection arthroplasty, redirection osteotomy, and arthrodesis have been proposed for the treatment of a painful dislocated hip when a relocation procedure is impossible.
Knee
Deformities of the knee in patients with cerebral palsy are difficult to evaluate and rarely occur in isolation. Pelvic, hip, knee, ankle, and foot deformities are interrelated. Thus, a careful physical examination of the entire lower extremity is essential when evaluating the knee in patients with cerebral palsy. Important knee deformities are discussed below.
Flexion deformity
Flexion is the most common knee deformity in patients with cerebral palsy and frequently occurs in ambulatory children. Spastic hamstrings, weak quadriceps, or a combination of both can cause isolated knee flexion. Patients with spastic hip flexors or weak hip extensors or both develop compensatory knee flexion that results in a “jump gait,” in which the hips, knees, and ankles are flexed.
Patients with weakened gastrocnemius–soleus muscles from cerebral palsy or Achilles tendon lengthenings, ambulate with knee flexion to accommodate for the relative overpull of the ankle dorsiflexion. The indications for hamstring lengthening are a straight leg raise of less than 70° or a popliteal angle of less than 135° in the absence of significant bony deformity. Care must be taken not to overlengthen the hamstrings because it can lead to excessive weakness and knee hyperextension gait.
Stiff knee gait
Stiff knee gait is common in patients with cerebral palsy. Cospasticity of the hamstrings and quadriceps causes a loss of knee flexion that leads to decreased power and difficulties with foot clearance during the swing phase of gait. Gait analysis can highlight the spastic muscle. A transfer of the distal rectus femoral tendon to the semitendinosus medially or iliotibial band laterally is recommended, depending on the presence of malrotation.
recurvatum of the knee
recurvatum of the knee is caused by a relative imbalance between the quadriceps and the hamstrings owing to several factors, including
(1) spasticity of the quadriceps and hamstrings in which the quadriceps is stronger;
(2) weakened hamstrings secondary to previous surgery, overlengthening, or transfer;
(3) gastrocnemius-soleus weakness; and
(4) ankle equinus. A significantly isolated recurvatum should be treated with bilateral long leg braces with a pelvic band with the knees locked in 20° of flexion and ankle stops at 5° of dorsiflexion. When hip control is achieved, the pelvic band can be removed, but long leg braces often are used for years until a stable knee is obtained. Flexion osteotomy for this condition is not recommended.
Foot
Foot deformities are common in patients with cerebral palsy, with approximately 70%–90% of children affected. The most common deformity is ankle equinus, with equinovarus and equinovalgus deformities being equally common. A foot deformity can have significant effects on the patient’s overall ambulatory level. Common foot deformities are described below.
Equinus deformity
Conservative treatment of equines consists of stretching, bracing, and occasionally casting. Soleus stretching for 6 h a day can prevent equinus onset. Bracing, especially at night, to prevent the foot from going into the equinus position is essential. Surgery typically is indicated when the ankle cannot be brought into the neutral position in an ambulatory child and when it leads to difficulties with hygiene, shoe wear, and standing rehabilitation in a nonambulatory child.
Varus or valgus deformity
Varus and valgus deformities can occur in association with an equinus deformity. Valgus is more frequent than varus. It also is important to determine whether the deformity is flexible or rigid because flexible deformities are more likely to be successfully treated nonoperatively with orthotics, shoe modifications, and operatively with soft-tissue procedures such as tendon lengthenings, releases, or transfers (usually of the abnormally active muscle). Patients with rigid varus and valgus deformities generally require bone procedures, such as calcaneal osteotomy, and subtalar or triple fusions.
Sometimes, the biomechanics of the hip, knee, and tibia also influence the onset and outcome of a foot varus or valgus deformity and should be carefully evaluated. Other common foot deformities in children seen with cerebral palsy are forefoot adduction, hallux valgus, and claw toes.
Occupational therapy for cerebral palsy
Occupational therapy can help with managing everyday activities and functions, like eating, getting dressed, and using the bathroom. It does so by improving physical and cognitive ability and fine motor skills.
How Does Occupational Therapy Help?
Occupational therapy helps people develop or recover the skills needed to lead independent, satisfying lives. The “occupation” in occupational therapy does not refer to one’s profession. Rather, it refers to the everyday activities that give life meaning.
For a child, these meaningful activities include playing and learning. Pediatric occupational therapy focuses on improving the child’s ability to play and learn, which is important for development and becoming independent.
For children with cerebral palsy, occupational therapy can help with muscle and joint coordination issues — issues that can make everyday tasks difficult. Some of these tasks include eating, brushing teeth, and bathing. Occupational therapy can help to improve physical, cognitive, and social abilities, as well as fine motor skills and posture. This therapy can also help address difficulties with processing sensory information.
Benefits of Occupational Therapy
Occupational therapy is beneficial for children with cerebral palsy in many ways.
By optimizing upper body function and improving the coordination of small muscles, occupational therapy can help children with CP master the basic activities of daily living.
Occupational therapy can help children by:
Increasing their chance for independence
Improving their ability to play and learn
Boosting their self-esteem and confidence
Helping them develop a workable routine
Giving them a sense of accomplishment
Improving their quality of life
Parents and caregivers spend a lot of time helping children with cerebral palsy perform basic day-to-day activities. As the child begins to see the benefits of occupational therapy, the parents and caregivers do, too.
Allowing them to watch their child improve and become independent
Each type of cerebral palsy presents different symptoms that may hinder a child’s ability to live independently and complete daily activities.
Occupational therapy can help with the following issues related to each type of CP:
Spastic – Muscle stiffness in the upper and/or lower limbs and jerky movements characterize spastic cerebral palsy. Among other things, this can lead to difficulty getting dressed, bathing, using the bathroom, eating, drinking, writing, and holding objects.
Athetoid – Children with athetoid cerebral palsy are unable to regulate muscle tone, which makes it difficult to control their movements. The trouble with grasping objects, posture, drooling, swallowing, and speaking are common among children with athetoid CP.
Ataxic – Problems with balance and coordination are common among children with ataxic cerebral palsy. These children often struggle with precise movements and have tremors or shakiness. This makes it difficult to perform tasks like writing or eating that require precise finger movements, or repetitive movements like clapping.
What to expect in occupational therapy
As with physical therapy and speech therapy, occupational therapy is different for every child with cerebral palsy. Each child’s occupational therapy treatment plan is highly individualized and tailored to their individual physical, intellectual, and social-emotional abilities.
During your child’s first therapy session, the occupational therapist will perform a complete evaluation. This includes testing the child’s fine motor, perceptual and oral-motor development, and observing how the child responds to touch and movement. The occupational therapist will also interview the parent to find out about the child’s strengths and weaknesses when performing daily activities, as well as pinpoint the specific goals for the child to work toward.
Most children with the cerebral palsy need to be reevaluated every six to nine months. After these evaluations, the occupational therapist will tweak the treatment plan accordingly based on progress and change.
Exercises Used in Occupational Therapy
Occupational therapy involves using functional activities to progressively improve functional performance.
Occupational therapy exercises focus on the following skill areas:
Fine Motor Control – Improves hand dexterity by working on hand muscle strength, finger isolations, in-hand manipulations, arching the palm, thumb opposition, and pincer grasp. Activities include squeezing a clothespin, playing with water squirt toys ,and pushing coins into the slot of a piggy bank.
Bilateral Coordination – Play/movements teach the child to control both sides of the body at the same time, like drumming, pushing a rolling pin ,and pulling apart construction toys (Legos).
Upper Body Strength and Stability – Play focuses on strengthening and stabilizing the trunk (core), shoulder ,and wrist muscles through exercises, such as crawling, lying on the tummy while reading, playing catch in a kneeling position ,and pouring water from a pitcher into a cup.
Crossing the Midline – These activities, like making figure eights with streamers and throwing balls at a target to the right or left of the center, teach the child to reach across the middle of their body with their arms and legs to the opposite side.
Visual Motor Skills – Improves hand-eye coordination through activities, like drawing, stringing beads or macaroni a,nd catching and throwing a ball.
Visual Perception – These activities improve the ability to understand, evaluate and interpret what’s being seen. Activities include alphabet puzzles, playing with different shapes, and matching games.
Self-Care – Improves the ability to perform activities of daily living and ppreparesthe child to be more independent at home, at school ,and in the community. Exercises can be as simple as practicing these ADLs, like brushing their teeth, getting dressed, and self-feeding.
Occupational therapists use specific techniques to help children reach their goals, including:
Pediatric Constraint Induced Movement Therapy (CIMT) – Improves the ability to move weaker parts of the body by restraining their stronger counterpart. For a child who has difficulty moving one of their arms, the stronger arm will be completely restrained for asome timewhile the weaker arm is strengthened and trained.
Sensory Integration Therapy – Improves the ability to receive, register, interpret and act on information that comes to the brain through sensory receptors. These activities provide the child with different sensory experiences and can include playing with balls, play dough, silly putty, sand, and water, walking on different carpet textures, and finger painting.
Equipment Used in Occupational Therapy
Many different tools and assistive devices are used in occupational therapy. Equipment can range from common household items to high-tech assistive technologies.
Adaptive scissors (with spring closures or grips for easier use)
Writing utensils
Splints
Adaptations to clothing (zipper pulls, button hooks, reachers)
Toys to help with the development of motor skills
Games and toys that help with motor and cognitive development
Assistive Devices
Pencil grips
Specialized feeding utensils
Seating and positioning equipment
Computer software and accessibility
Household aids and equipment
School chairs and tables
Toilet and bathing aids
Tablets
Occupational Therapy by Age
Occupational therapy helps people of all ages. For children with cerebral palsy, treatment will be based on the child’s physical, intellectual, social, and language abilities, as well as their age.
Toddlers – Treatment for toddlers revolves around play and learning. Games and toys are used to improve the child’s cognitive and physical development.
Young Children – Therapy for young children works on improving cognitive and physical development, as well as the child’s ability to perform daily living activities. Occupational therapy can also improve the child’s performance in school and their socialization skills.
Speech therapy for cerebral palsy
Speech and language therapy can help improve communication, eating, and swallowing. It can also encourage confidence, learning, and socialization.
How does speech therapy help?
Speech disorders are common among those with cerebral palsy. A 2012 study conducted by Swedish researchers found that speech problems affect more than half of all children with cerebral palsy.
Some children with cerebral palsy have difficulty controlling the muscles in their face, throat, neck a,nd head. This can lead to trouble with speech, chewing, and swallowing. It can also cause drooling and affect the overall ability to interact and learn. Those who also have difficulty hearing may have a hard time understanding spoken language.
Speech and language therapy seeks to improve a child’s speech and communication by strengthening the muscles used for speech, increasing oral motor skills, and by improving their understanding of speech and language. It also can help with swallowing disorders, like dysphagia.
Benefits of speech therapy
Speech therapy can be very beneficial for children with cerebral palsy.
As children improve their speech and communication, they are better able to express their needs, share their thoughts and interact with others.
Children with cerebral palsy who have difficulty eating, chewing a, nd swallowing may also have a problem with normal growth and maintaining a healthy weight. Speech therapy can help with these issues, making it easier for the child to get the proper nutrition and hydration they need. This can improve their overall quality of life and increase their independence. Speech therapy can help with the following:
Articulation
Pronunciation
Fluency/stuttering
Sound and word formation
Listening
Pitch
Language and vocabulary development
Speech volume
Word comprehension
Word-object association
Breath support and control
Chewing
Swallowing
Speech muscle coordination and strength
The benefits of speech therapy go beyond improving a child’s ability to understand and use language. Communication is very important to other areas of development, like cognitive development and social and emotional development. As the child learns to better express themselves, the benefits can be seen in many other aspects of their life and development.
Speech therapy is beneficial because it can help:
Encourage learning and education
Improve ability to problem-solve
Increase independence
Improve literacy
Improve ability to express thoughts and ideas
Improve socialization
Boost self-esteem
Reduce shyness
Improve the quality of life
Improve swallowing function and safety
Children with different types of cerebral palsy may face communication problems, which speech therapy can help treat.
Different speech issues as they relate to each different type of cerebral palsy include:
Spastic – Children with spastic cerebral palsy usually struggle with slow, imprecise oral movements that require a lot of effort. Their speech often sounds slurred and their voice sounds tight or hoarse.
Athetoid – Those who have athetoid cerebral palsy often have a hard time controlling their face and tongue muscles. They also have difficulty controlling their breathing and vocal cords and have problems with eating and drooling.
Ataxic – “Scanning” speech, which is speaking in a monotone voice with breathy sounds, is common among children with ataxic cerebral palsy. Their speech is often marked by pauses and accelerations and they also have difficulty swallowing.
What to expect in speech therapy
Speech therapy is different for every child with cerebral palsy. During the first session, the speech therapist will perform an initial assessment of the child’s physical and cognitive functioning. This assessment may include an examination of the child’s case history, an oral cavity exam, audiology tests, articulation assessments, language and fluency assessments, and cognitive assessments.
After the original assessments, the speech therapist can then determine the child’s diagnosis and create a treatment plan. Treatment usually consists of exercises tailored to the child’s specific struggles with communication or swallowing. Assistive communication devices and sign language are often used to help the child express himself or herself. These are especially helpful in more severe cases, such as when children are completely nonverbal.
Exercises used in speech therapy
Many different exercises are used in speech therapy. Each child’s treatment plan will be different based on their challenges and needs.
Some examples of common exercises for speech therapy include:
Articulation therapy – Using language cards to help focus on specific sounds; encouraging children to make sounds while looking in the mirror to help them understand how their mouth moves.
Blowing exercises – Blowing bubbles or a whistle to train the mouth muscles to produce certain sounds and strengthen the abdominals for breath control.
Breathing exercises – Working on inhalation and exhalation to strengthen the diaphragm.
Jaw exercises – Eating foods that require extra chewing, like celery, apples, and carrots, to strengthen jaw muscles; practicing opening and shutting their mouth using only the jaw muscles while someone else holds their chin.
Language and word association – Using flashcards with different words and sounds written on them; putting together puzzle pieces with words that go together, like “sock” and “shoe,” “toothbrush” and “toothpaste,” and “bat” and “ball.”
Lip exercises – Squeezing their lips around a lollipop to increase strength; pursing their lips to improve lip extension.
Swallowing exercises – Doing an “effortful swallow,” which is collecting liquid or saliva in the mouth and swallowing it in one gulp. This helps prevent food and fluids from falling into the airway. Doing a “masako maneuver,” which strengthens the muscles in the back of the throat. This is done when the child sticks their tongue out, gently puts pressure on it with their teeth to hold it in place, and then practices swallowing.
Tongue exercises – Strengthening the tongue by sticking it out and pushing it against a tongue depressor or spoon for seconds at a time.
Equipment used in speech therapy
Speech therapists use a variety of different tools to help children with cerebral palsy improve or overcome their communication struggles. Assistive technology, or assistive devices, is also used as communication aids, especially for nonverbal children.
Tools
Tools commonly used in speech therapy include:
Placement tools (correct tongue positioning for certain sounds)
Oral sensory chews
Straws
Tongue depressors
Picture boards
Books
Flashcards
Dry erase boards
Flip charts
Assistive devices
The following assistive devices are commonly used to help those with communication issues:
Tablets
Computers and keyboards
Augmentative and alternative communication devices (AAC)
Unaided communication systems — using the child’s body to communicate a message, like body language or sign language
Aided communication systems — tools in addition to the child’s body, like paper and pencils, boards, speech-generating devices, etc.
Specialized software
Speech therapy by age
As the child gets older or improves their abilities, their speech therapy treatment plan must change accordingly. The first three years of a child’s life are extremely important for acquiring speech and language skills because their brain is developing and maturing, allowing it to easily absorb this information. Early intervention gives a child the best chance to develop and learn at their full potential.
Toddlers — Speech therapy for toddlers is play-based with games and toys, the repetition of noises and words, singing songs, and arts and crafts.
Young children — For school-aged children, there’s an extra emphasis on social interaction, although games and toys are still used. Therapy usually consists of different activities to promote communication, like storytelling, having conversations, repetition of sounds and words, and working on the child’s school work. Therapy also helps the child improve their social skills, such as keeping their head up and maintaining eye contact while talking.
Alternative therapy
Caring for a child with cerebral palsy requires a multifaceted approach. Alternative treatment methods are used in addition to traditional therapy
How can alternative therapy help?
For many children and adults with cerebral palsy, therapy programs are an essential part of managing symptoms and improving overall mobility.
Doctors and specialists will often recommend starting with traditional CP therapy options, such as physical, occupational, and speech therapy. These therapies generally allow for improved mobility, speech, and overall independence.
However, each case of cerebral palsy is different. For this reason, your child’s therapy and treatment plan should be based on their symptoms and mobility limitations. Those with more severe types of CP or coexisting conditions may respond better to complementary or alternative types of therapy.
The medical term “Complementary and Alternative Therapy” describes a set of treatment methods that are not presently considered to be traditional CP treatment (i.e., physical, occupational, and speech therapy).
The term “complementary therapy” refers to therapy that is used in addition to conventional therapy. “Alternative therapy” refers to therapy that replaces conventional CP therapy.
Complementary and alternative therapy options for CP include:
Hippotherapy
Music therapy
Aquatic therapy
Acupuncture
Several benefits stem from alternate treatment methods. Your doctor may recommend adding an alternative therapy program to your child’s existing treatment plan, or they may suggest utilizing another treatment method entirely. A CP specialist will be able to recommend the best therapy options available based on your child’s diagnosis, performance, and progress.
Hippotherapy
Hippotherapy is a form of therapy used to improve muscle tone and mobility. Contrary to its name, this therapy doesn’t require any hippos, but rather – horses.
Hippotherapy involves horseback riding and channeling a horse’s natural movement to improve mobility and posture over time. Hippotherapy is also referred to as “equine therapy”.
Horses exert patterns of movement and rhythm as they trot, which forces the rider’s torso and hips to mimic this movement to stay mounted on the horse. In turn, this allows the joints, muscles, and bones to become properly aligned.
Working consistently to improve an individual’s natural motor responses over a series of therapy sessions, can help overall movement while off-horse.
Benefits of hippotherapy for cerebral palsy
Several positive results can stem from utilizing hippotherapy for CP treatment. Hippotherapy can be used to improve:
Abnormal muscle tone
Impaired coordination
Decreased mobility
Poor posture
Impaired balance
Impaired limbic system function
In a study performed on hippotherapy in 2002, 17 children with CP were asked to ride for 1 hour per week for 18 weeks. It was concluded that all children exhibited improvement, specifically in the walking, running, and jumping portions. It was also noted that these improvements lasted at least 16 weeks after the therapy was completed.
In addition to the physical benefits of hippotherapy, there are also many ways that this therapy can be used to enhance mental health and communication. Horses are thought to be physically, psychologically, and emotionally comforting animals.
There is a bond that often develops between a rider and a horse. This can provide an important source of motivation, confidence, and encouragement for an individual with CP.
Music therapy
Common symptoms of cerebral palsy are issues related to cognitive functioning, speech, and motor skills. Music therapy can be used to enhance these areas and allow for improved functioning overall.
According to the American Music Therapy Association (AMTA), music therapy is defined as the emerging, evidence-based use of sound and rhythm to establish a therapeutic relationship between an individual and their therapist.
Benefits of music therapy for cerebral palsy
Music therapy utilizes an array of exercises to improve an individual’s CP symptoms. Music therapy can improve:
Motor skills
Coordination
Communication skills
Language processing
Auditory responses
Relaxation
Range of motion
Music is an effective platform to manage many of the symptoms of CP. During music therapy, children will work with a music therapist to complete an array of fun, interactive activities. This often encompasses singing, playing instruments, dancing to the beat, composing songs, and listening to certain sounds or words.
Music therapy is closely related to enhanced cognitive functioning. Research has shown that music therapy can increase alertness because the beat of the music helps the brain form meaningful neuro connections related to concentration and focus. This helps individuals with CP function better with and without music present.
Aquatic therapy
For children with severe types of CP or mobility limitations, aquatic therapy can be a very beneficial option. When compared to traditional physical therapy, water-based exercise offers a fun, less intimidating alternative.
Aquatic therapy entails performing a series of exercises while in the water, such as length swimming, shallow-water tuck jumps, stride jumps, jumping jacks, and wall-and-sit kicking.
When immersed in water, individuals with CP will be able to perform an array of exercises that may not be possible on land, such as jumping jacks. This is due to the way that water reduces pressure on muscles, bones, and joints — allowing for free movement.
Benefits of aquatic therapy for cerebral palsy
Several physical and cognitive benefits can come from aquatic therapy. This type of therapy can be used to improve:
Flexibility
Respiratory function
Muscle strength
Gait
Coordination
Endurance
Over the years, there has been much research conducted regarding the advantages of using aquatic therapy for CP treatment. One study published in 2007 set out to examine the effects of water therapy on individuals with limited mobility.
Researchers studied the way that 37 children with delayed mobility reacted to different types of therapy. Half of the children were prescribed water therapy, while the others were prescribed traditional physical therapy on land. The study concluded that the water therapy group exhibited improved balance, weakness, and mobility when compared to those who received traditional physical therapy.
Acupuncture
Cerebral palsy is often associated with back pain, joint inflammation, muscle weakness, and neck pain. To reduce this pain and discomfort, many children and adults with cerebral palsy have turned to acupuncture.
Acupuncture is a form of complementary therapy. This means that when used in addition to traditional therapy sessions, acupuncture can significantly improve neurological functioning and muscle hypertonicity.
Acupuncture originated in China, where it has been used to prevent and treat diseases for thousands of years. Acupuncture treatment is typically given 2 to 3 times a week for about 10 total sessions.
This therapy involves the insertion of fine needles into the body at specific entry points. When used for CP treatment, acupuncture needles will generally be placed in defined areas on the scalp, ears, fingers, arms, legs, and feet.
Benefits of acupuncture for cerebral palsy
While acupuncture has long been recognized as an effective treatment method by the Chinese, it has only gained popularity in the U.S. over the last 40 years. Acupuncture can be used to improve:
Weakness of legs, arms, and hands
Loss of speech (aphasia)
Loss of voluntary movement (ataxia)
Loss of hearing
Pain caused by the central nervous system
Balance and coordination
In a study from 2012, it was found that acupuncture can improve or remove some symptoms of CP in children. Michael, a 6-year-old patient with CP, was the subject of the study and was treated using acupuncture for 15 total sessions.
Before acupuncture, Michael’s parents reported that he had never spoken a full sentence and had almost no coordination in his upper or lower limbs — despite several years of traditional therapy. By the end of the study, Michael was able to speak in full sentences, and voluntarily move his body and limbs, and his math and reading scores progressed by a grade level.
While Michael’s experience with acupuncture displays an important medical advancement for alternative CP treatment options, this type of therapy should only be used when recommended by your child’s doctor. Additionally, it is important to note that acupuncture is a complementary therapy and should be used in addition to traditional therapies.