
Spinal cord injury (SCI) is damage to the spinal cord that causes temporary or permanent changes in its function. Symptoms may include loss of muscle function, sensation, or autonomic function in the parts of the body served by the spinal cord below the level of the injury. Injury can occur at any level of the spinal cord and can be a complete injury, with a total loss of sensation and muscle function, or incomplete, meaning some nervous signals are able to travel past the injured area of the cord. Depending on the location and severity of the damage, the symptoms vary, from numbness to paralysis to incontinence. Long-term outcomes also range widely, from full recovery to permanent tetraplegia (also called quadriplegia) or paraplegia. Complications can include muscle atrophy, pressure sores, infections, and breathing problems.
Causes
Most spinal cord injuries are preventable, and knowing the causes of these injuries can help you avoid becoming a victim. And if you or someone you love already deal with the frustration and pain of a spinal cord injury, knowing the most common sources of these injuries can help you feel a bit less alone.
The National Spinal Cord Injury Statistical Center at the University of Alabama-Birmingham conducts annual spinal cord injury research, including an assortment of statistics on SCI injuries. It’s interesting to note that, in almost all categories of injuries, men are more likely to be injured than women.
In 2018, the most recent year for which statistics are available, the 10 leading causes of spinal cord injuries, and their percentage of the total number of injuries, were as follows:
- Auto Accidents: Nationwide, car accidents claim more than 32,000 lives annually. Unsurprisingly, then, car accidents are the leading cause of spinal cord injuries, accounting for 7,205 (29.3%) male injuries and 2,402 (48.3%) female injuries in 2014. Find out what to do after a car accident.
- Falls: Falls were the second-leading cause of SCI in 2014, accounting for 5,406 (22%) of male injuries and 1,262 (21.5%) of female injuries.
- Gunshot Wounds: Gun-related injuries accounted for 4,163 (16.9%) of male SCIs in 2014, and 572 (9.1%) of female injuries.
- Diving Injuries: Propelling headfirst into the water is an inherently dangerous activity. 1,718 (7%) men suffered spinal cord injuries due to diving accidents in 2014, with 122 (2.1%) female divers experiencing an SCI.
- Motorcycle Accidents: The lack of external protection means that even minor motorcycle collisions can be deadly. In 2014, 1,695 (6.9%) men suffered spinal cord injuries while on motorcycles, with a mere 145 (2.5%) women experiencing such injuries.
- Falling Objects: Those in industries where falling objects are common are especially vulnerable. 822 men (3.3%) and 37 women (.6%) experienced spinal cord injuries due to falling objects in 2014.
- Medical and Surgical Complications: Choosing the right doctor, and carefully monitoring any unusual symptoms can help you avoid a medically induced SCI. 537 (2.2%) men suffered spinal cord injuries due to medical complications in 2014.
- Pedestrian Injuries: Ample research suggests that pedestrians are often distracted by phones and other devices, and many such pedestrians are in denial about the extent of their distraction. In 2014, 357 (1.5%) men suffered pedestrian-related spinal cord injuries, with 131 women (2.2%) meeting a similar fate.
- Bicycle Accidents: Helmets save lives. Over time, fatal bicycle accidents have generally declined, suggesting that helmet laws are working to keep cyclists safe. Nevertheless, 409 men (1.7%) and 49 women (.8%) suffered bicycling-related spinal cord injuries in 2014.
- Other SCI Injury Causes:
- Unclassified, which includes injuries that don’t fit neatly into a single category, or for which adequate data is not available.
- Penetrating wounds, such as an object entering the brain or spinal cord.
- All-terrain vehicle (ATV) accidents.
- Accidents in other vehicles, such as jet skis and boats.
- Snow skiing.
- Football.
- Winter sports such as snowboarding.
- Horseback riding.
- Surfing, including body surfing.
- Other sports-related injuries.
Standard Symptoms
Signs and symptoms of a spinal cord injury may present immediately or some symptoms may be delayed as swelling and bleeding occur in or around the spinal cord. One or more of the following symptoms may occur with a spinal cord injury:
- Pain and numbness, or burning sensation
- Inability to move the extremities or walk
- Inability to feel pressure, heat, or cold
- Muscle spasms
- Loss of bladder or bowel control
- Difficulty breathing
Symptoms by Region
There are three main areas in which a person may suffer spinal cord injury: cervical, thoracic, and lumbar. The fourth section of the spine (sacral), does not contain spinal cord tissue. Consequently, though you may cause damage to the sacral vertebrae or nerves, you will not damage the cord at that level.
-
Cervical (C1-C8) – Damage to the spinal cord in the cervical spine is considered the most severe because it can be life-threatening. Symptoms of cervical spinal cord damage may affect the arms, legs, mid-body, and even the ability to breathe on one’s own. The higher up in the cervical spine the damage occurs, the worse the injury. Symptoms may be felt on one or both sides of the body.
-
Thoracic (T1-T12) – Damage to the spinal cord in the thoracic spine typically affects the legs. Thoracic spinal cord damage high up in the area may affect blood pressure.
-
Lumbar (L1-L5) – Damage to the spinal cord in the lumbar spine typically affects one or both legs. Patients with lumbar spinal cord damage may also have trouble controlling their bladder and/or bowel function.
Types of Spinal Cord Injuries
All spinal cord injuries are divided into two broad categories: incomplete and complete.
- Incomplete spinal cord injuries – With incomplete injuries, the cord is only partially severed, allowing the injured person to retain some function. In these cases, the degree of the function depends on the extent of the injuries.
- Complete spinal cord injuries – By contrast, complete injuries occur when the spinal cord is fully severed, eliminating function. Though, with treatment and physical therapy, it may be possible to regain some function.
Incomplete spinal cord injuries are increasingly common, thanks in part to better treatment and increased knowledge about how to respond—and how not to respond—to a suspected spinal cord injury. These injuries now account for more than 60% of spinal cord injuries, which means we’re making real progress toward better treatment and better outcomes.
Some of the most common types of incomplete or partial spinal cord injuries include:
- Anterior cord syndrome – This type of injury, to the front of the spinal cord, damages the motor and sensory pathways in the spinal cord. You may retain some sensation but struggle with movement.
- Central cord syndrome – This injury is an injury to the center of the cord, and damages nerves that carry signals from the brain to the spinal cord. Loss of fine motor skills, paralysis of the arms, and partial impairment—usually less pronounced—in the legs are common. Some survivors also suffer a loss of bowel or bladder control or lose the ability to sexually function.
- Brown-Sequard syndrome – This variety of injury is the product of damage to one side of the spinal cord. The injury may be more pronounced on one side of the body; for instance, the movement may be impossible on the right side, but maybe fully retained on the left. The degree to which Brown-Sequard patients are injured greatly varies from patient to patient.
Knowing the location of your injury and whether or not the injury is complete can help you begin researching your prognosis and asking your doctor intelligent questions. Doctors assign different labels to spinal cord injuries depending upon the nature of those injuries. The most common types of spinal cord injuries include:
- Tetraplegia – These injuries, which are the result of damage to the cervical spinal cord, are typically the most severe, producing varying degrees of paralysis of all limbs. Sometimes known as quadriplegia, tetraplegia eliminates your ability to move below the site of the injury and may produce difficulties with bladder and bowel control, respiration, and other routine functions. The higher up on the cervical spinal cord the injury is, the more severe symptoms will likely be.
- Paraplegia –This occurs when sensation and movement are removed from the lower half of the body, including the legs. These injuries are the product of damage to the thoracic spinal cord. As with cervical spinal cord injuries, injuries are typically more severe when they are closer to the top vertebra.
- Triplegia – Triplegia causes loss of sensation and movement in one arm and both legs, and is typically the product of an incomplete spinal cord injury.

www.rxharun.com
Anatomy of Spinal Cord Injury
Defined as spinal cord injury with some preserved motor or sensory function below the injury level including
- voluntary anal contraction (sacral sparing)
- sacral sparing critical to separate complete vs. incomplete injury
- OR palpable or visible muscle contraction below the injury level
- OR perianal sensation present
Epidemiology
11,000 new cases/year in the US
- 34% incomplete tetraplegia
- central cord syndrome most common
- 17% incomplete paraplegia
- remaining 47% are complete
- Prognosis most important prognostic variable relating to neurologic recovery is the completeness of the lesion (severity of neurologic deficit)
Nervous system
Central nervous system
- includes the brain & spinal cord the spinal cord ends at L3 at birth and L1 at maturity
Peripheral nervous system’ contains the
- cranial nerves
- peripheral nerves
Autonomic nervous system > sympathetic system
A total of 22 ganglia (3 cervical, 11 thoracics, 4 lumbar, 4 sacral) > cervical ganglia
- the three cervical include the stellate, middle, and superior
- the middle ganglion is most at risk at the level of C6 where it lies close to the medial border of the longus colli muscles
- injury to the middle ganglion/sympathetic chain will lead to Horner’s syndrome
Parasympathetic nervous system
- hypogastric plexus formed by S2, S3, S4 parasympathetic fibers and lumbar sympathetic fibers (splanchnic nerves)
The spinal cord extends from the brainstem to the inferior border of L1
- conus medullaris is the termination of the spinal cord
- filum terminal is a residual fragment of the spinal cord that extends from conus medullaris to sacrum.
- thecal sac the dural surrounded sac that extends from the spinal cord and contains CSF, nerve roots and the cauda equina
- cauda equina nerve roots and filum terminal surrounded by dura that extend from the spinal cord
Embryology of the spinal cord
Neural Tube
- becomes spinal cord
- formed from the primitive Streak, which turns into the primitive (midsagittal) groove > which turns into the Neural Tube
- failure of the neural tube to close leads to
- anencephaly when it fails to close cranially
- spinal Bifida occulta, meningocele, myelomeningocele when it fails to close distally
Neural crest
Forms dorsal to neural tube becomes the
- peripheral nervous system
- pia mater
- spinal ganglia
- sympathetic trunk
Notochord
Forms ventral to neural tube >becomes
- vertebral bodies
- intervertebral discs
- nucleus pulposus from cells of the notochord
- annulus from sclerotome cells associated with segmentation
Layers of the spinal cord
Layers of the spinal cord include the
- dura mater (outside)
- arachnoid
- pia mater (inside)
When viewed in cross-section, the spinal cord is divided into gray matter and white matter.
Gray matter:
- H- or butterfly-shaped area in the center of the cord
- Consists of the neuronal cell bodies
- Site of synaptic connections between neurons
- Dorsal horns (posterior):
- Gives rise to the dorsal roots at the dorsolateral surface of the cord
- Consists of sensory neurons
- Ventral horns (anterior):
- Gives rise to the ventral roots at the ventrolateral surface of the cord
- Consists of motor neurons:
- Neurons that innervate proximal muscles are medial
- Neurons that innervate distal muscles are lateral
- Lateral horns (anterolateral):
- Also called the intermediolateral columns
- Found only in the thoracic and lumbar regions
- Contains neurons of the sympathetic nervous system
- Send out axons via the ventral roots
- Gray commissure:
- Central area where the right and left halves cross over
- Contains the central canal (collapsed in most areas in the adult)
White matter:
- Area surrounding the gray matter
- Consists of myelinated neuronal axons
- Composed of bundles of axons called tracts
- Organized into:
- Columns (funiculi):
- Dorsal (posterior) column
- Lateral column
- Ventral (anterior) column
- Columns are subdivided into fasciculi or tracts.
- Columns (funiculi):
Spinal meninges
The meninges are the fibrous membranes that encase the spinal cord (and brain). The 3 layers and 2 defined spaces between/around the layers are (from outside to inside):
- Dura mater:
- Outermost membrane of the spinal cord
- Forms a long tubular sheath around the spinal cord within the vertebral canal called the dural sheath
- Composed mainly of tough fibrous tissue, with some elastic fibers
- Epidural space:
- The space outside the dura mater, between dura mater and periosteum of the vertebral bone
- Occupied by small vessels and adipose and loose connective tissue
- Arachnoid mater:
- Delicate, avascular membrane
- Composed of simple squamous epithelium
- Adheres to the dura mater
- Subarachnoid space:
- Space between the arachnoid mater and pia mater
- Contains: CSF and a web of collagenous and elastic tissue (connecting the pia mater and arachnoid mater)
- Pia mater:
- Innermost membrane, in direct contact with the spinal cord
- Thin and transparent
- Closely follows all the surface features of the spinal cord
- Directly covers the roots of the spinal nerves and the spinal blood vessels
- Inferior to the conus medullaris, the pia mater continues as the filum terminale.
Spinal Cord Functional Tracts
- dorsal columns (posterior funiculi)
- deep touch, proprioception, vibratory
- lateral spinothalamic tract
- pain and temperature
- a site of chordotomy to alleviate intractable pain
- ventral spinothalamic tract
- light touch
- Descending Tracts (Motor
lat) lateral corticospinal tract- main voluntary motor
- upper extremity motor pathways are more medial(central) which explains why a central cord injury affects the upper extremities more than the lower extremities
- ventral corticospinal tract
- voluntary motor
- main voluntary motor
Blood Supply of the spinal cord
spinal cord blood supply provided by
- anterior spinal artery
- primary blood supply of anterior 2/3 of the spinal cord, including both the lateral corticospinal tract and ventral corticospinal tract
- posterior spinal artery (right and left)
- primary blood supply to the dorsal sensory columns
- Artery of Adamkiewicz
- the largest anterior segmental artery
- typically arises from a left posterior intercostal artery, which branches from the aorta, and supplies the lower two-thirds of the spinal cord via the anterior spinal artery
- significant variation exists
- in 75% it originates on the left side between the T8 and L1 vertebral segments
Cerebral Spinal Fluid
unction
- a colorless fluid that occupies the subarachnoid space surrounding the brain, spinal cord, and ventricular system
- the subarachnoid space is between the arachnoid mater and pia mater
- provides mechanical and immunological protection for the brain, spinal cord, and thecal sac
Production
- location
- most human cerebrospinal fluid (CSF) is produced by the choroid plexus in the third, fourth, and lateral ventricles of the brain.
- CSF is an ultrafiltrate of blood plasma through the permeable capillaries of the choroid plexus
- volume
- total CSF volume between the brain, spinal cord, and the thecal sac is ~150 mL
- CSF formation occurs at a rate of ~500mL per day
- thus the total amount of CSF is turned over 3-4 times per day
Nerve Root Anatomy
Cervical spine
- nerve roots exit above the corresponding pedicle
- C5 nerve root exits above the C5 pedicle
- nerve root travels horizontally to exit
- there is an extra C8 nerve root
- that does not have a corresponding vertebral body
Thoracic Spine
- nerve root travel below the corresponding pedicle
- T1 exits below T1 pedicle
- T12 exits below T12 pedicle
Lumbar spine
- nerve roots descend vertically before exiting
- nerve root travel below the corresponding pedicle
- L1 exits below L1 pedicle
- L5 exits below L5 pedicle
Ascending Tracts (motor)
- lateral corticospinal tract (LCT)
- ventral corticospinal tract
Ascending tracts (sensory)
- dorsal columns
- deep touch
- vibration
- proprioception
- lateral spinothalamic tract (LST)
- pain
- temperature
- ventral spinothalamic tract (VST)
- light touch
Clinical classification
- anterior cord syndrome (see below)
- Brown-Sequard syndrome
- central cord syndrome
- posterior cord syndrome
- Conus medullaris syndrome
- Cauda equina syndrome : which involves damage to nerve roots at the caudal end of the cord, is not a spinal cord syndrome. However, it mimics conus medullaris syndrome, causing distal leg paresis and sensory loss in and around the perineum and anus (saddle anesthesia), as well as bladder, bowel, and pudendal dysfunction (eg, urinary retention, urinary frequency, urinary or fecal incontinence, erectile dysfunction, loss of rectal tone, abnormal bulbocavernosus and anal wink reflexes). In cauda equina syndrome (unlike in spinal cord injury), muscle tone and deep tendon reflexes are decreased in the legs.
- Spinal Contusions: The most common type of spinal cord injury. The spinal cord is bruised but not severed. Inflammation and bleeding occur near the injury as a result of the injury.
- Injuries to Individual Nerve Cells: Loss of sensory and motor functions in the area of the body to which the injured nerve root corresponds.
Flexion Fracture Pattern
Complete and Incomplete Spinal Cord Injury
The terms, ‘Complete,’ and, ‘Incomplete,’ in reference to a spinal cord injury is associated with the type of lesion in the person’s spine.
- A person who is completely paralyzed below the lesion has a, ‘Complete,’ SCI.
- A person who experiences partial paralysis below the lesion on their spine has an, ‘Incomplete,’ SCI.
Persons with incomplete SCI might have some sensation below the lesion, yet have no movement. There are a number of types of incomplete spinal cord injuries. Every person with an incomplete spinal cord injury is unique in regards to their injury.
- Compression fracture: While the front (anterior) of the vertebra breaks and loses height, the back (posterior) part of it does not. This type of fracture is usually stable and rarely associated with neurologic problems.
- Axial burst fracture: The vertebra loses height on both the front and back sides. It is often caused by a fall from a height and landing on the feet.
Extension Fracture Pattern
- Flexion/distraction (Chance) fracture: The vertebra is literally pulled apart (distraction). This can happen in accidents such as a head-on car crash, in which the upper body is thrown forward while the pelvis is stabilized by a lap seat belt.
Rotation Fracture Pattern
- Transverse process fracture: This fracture is uncommon and results from rotation or extreme sideways (lateral) bending, and usually does not affect stability.
- Fracture-dislocation: This is an unstable injury involving bone and/or soft tissue in which a vertebra may move off an adjacent vertebra (displaced). These injuries frequently cause serious spinal cord compression.
- method to scale ASIA classification
Grading Scales
There are two well-known scales used to grade and prognosticate SCI. The Frankel scale was developed during World War I, but is less commonly used today. It is a basic scale that grades the SCI based on level and is used to evaluate functional recovery. There are five grades used in the Frankel scale, which essentially divide completely versus incomplete spinal injuries as follows:
- A — complete paralysis (no motor/sensory below level of injury);
- B — sensory present below the level of injury;
- C — incomplete injury with motor and sensory function below the level of injury;
- D — fair to good motor function below the level of injury; and
- E — normal function (no motor of the sensory deficit).3
The American Spinal Injury Association (ASIA) Impairment Scale (AIS) is a more widely used and more refined scale. Based on the Frankel scale’s five grading levels, the AIS was originally developed in 1982 and has undergone six revisions, with the most recent occurring in 2002. The AIS differs from the Frankel scale in that it more clearly defines complete and incomplete injury by determining sacral sparing (presence of rectal motor function or sensory function at S4-S5 dermatome), determining the presence of neurologic level of injury using sensory and motor evaluation in bilateral extremities, and by determining, in incomplete injuries, where partial zones of sensory or motor preservation exist.
Central Cord Syndrome
The most common of all partial cord syndromes is central cord syndrome, which is distinguished from the other cord syndromes by the fact that the upper extremities are significantly more affected from the motor perspective than the lower extremities are. The most common mechanism of injury is a hyperextension injury, and it is usually seen after a fall in an older population with preexisting spinal stenosis or arthritis. The injury to the spinal cord affects the central portions of the corticospinal and spinothalamic tracts, resulting in a disproportionate pattern of symptoms between the upper and lower extremities. Patients typically have greater weakness in the proximal muscles than in the distal ones. Sensory symptoms are also appreciable, with some patients presenting with dysesthesias of their upper extremities as their predominant symptom.
Epidemiology
Pathophysiology
- believed to be caused by spinal cord compression and central cord edema with selective destruction of lateral corticospinal tract white matter
- anatomy of the spinal cord explains why upper extremities and hands are preferentially affected
- hands and upper extremities are located “centrally” in the corticospinal tract
Symptoms
- the weakness with hand dexterity most affected
- hyperpathia
- burning in distal upper extremity
physical exam
- loss
- motor deficit worse in UE than LE (some preserved motor function)
- hands have a more pronounced motor deficit than arms
- preserved
- sacral sparing
Late clinical presentation
- UE have LMN signs (clumsy)
- LE has UMN signs (spastic)
Treatment
- nonoperative vs. operative
- extremely controversial
- good prognosis although full functional recovery rare
- usually ambulatory at final follow up
- usually, regain bladder control
- upper extremity and hand recovery is unpredictable and patients often have permanent clumsy hands
Recovery occurs in a typical pattern
- lower extremity recovers first
- bowel and bladder function next
- proximal upper extremity next
- hand function last to recover
Anterior Cord Syndrome
Anterior cord syndrome is usually sustained due to a hyperflexion injury to the cervical cord but can occur anywhere in the spinal column. Hyperflexion of the cord causes direct contusion to the cord or can result in the protrusion of disc contents, bony fragments that have fractured, or, rarely, can cause direct laceration or thrombosis to the anterior spinal artery. Since the injury to the cord is bilateral, the pattern of symptoms that accompany this injury includes bilateral motor paralysis and loss of pinprick, temperature, and pain sensation below the level of injury. Since the posterior aspect of the cord is preserved, so is proprioception and vibratory sensation.
The overall prognosis for anterior cord syndrome is poor. Improvement in motor function can be seen within the first 24 hours following injury, but usually does not occur after the first day. After 30 days following injury, there is little to no additional recovery of function.
A condition characterized by
- motor dysfunction
- dissociated sensory deficit below the level of SCI
Pathophysiology >Injury to anterior spinal cord caused by
- direct compression (osseous) of the anterior spinal cord
- anterior spinal artery injury
- anterior 2/3 spinal cord supplied by the anterior spinal artery
Mechanism
- usually, result of flexion/ compression injury
- lower extremity affected more than upper extremity
- loss
- LCT (motor)
- LST (pain, temperature)
- preserved
- DC (proprioception, vibratory sense)
Prognosis
- worst prognosis of incomplete SCI
- most likely to mimic complete cord syndrome
- 10-20% chance of motor recovery
Brown-Séquard Syndrome
Brown-Séquard syndrome is an anatomic or functional hemisection of the cord, which has several potential causes. From a trauma perspective, Brown-Séquard is commonly the result of penetrating trauma to the spinal cord. However, more commonly it is due to inherent spinal or compressive lesions such as tumors or epidural hematomas. Classic Brown-Séquard syndrome, in its purest form, is described as a loss of ipsilateral motor function, proprioception, vibratory and pressure sensation, and contralateral loss of temperature and pain sensation below the level of injury. Although the pure form of Brown-Séquard syndrome is rarely seen, a partial form of Brown-Séquard is more common. Interestingly, because the fibers of the lateral spinothalamic tract decussate one or two levels above or below where the injury may occur, it is possible to see ipsilateral pain and temperature sensory loss above the level of injury.
Caused by complete cord hemitransection
- usually seen with penetrating trauma
Exam
- ipsilateral deficit
- contralateral deficit
- LST
- pain
- temperature
- spinothalamic tracts cross at spinal cord level (classically 2-levels below)
Prognosis
- excellent prognosis
- 99% ambulatory at final follow up
- best prognosis for function motor activity
Posterior Cord Syndrome
Introduction
- very rare
Exam
- loss
- proprioception
- preserved
- motor, pain, light touch
Neurological History and Examination
Taking a detailed history and performing a careful examination can help the doctor to determine the site of a specific neurological lesion and reach a diagnosis, or at least differential diagnoses. A systematic approach is required.
This is a general article, attempting to cover all aspects of neurological history and examination. You are referred to other related articles were relevant for more detail.
Mental state examination may also be an important consideration and this is covered in the separate Mini-Mental State Examination (MMSE) article.
Diagnosis
Observation of the patient
Gait
- Look at the patient’s gait as they enter the room.
- Note if there evidence of, for example, hemiparesis, foot drop, ataxic gait, a typical Parkinsonian gait.
- See separate Abnormal Gait and Gait Abnormalities in Children articles.
Speech
- Note any problem with articulation (dysarthria). Here comprehension is retained and speech construction is normal. There is usually weakness or incoordination of the orolingual muscles. Ask the patient to say ‘West Register Street’ if you are uncertain.
- Note any problem with phonation (dysphonia). This is usually due to laryngeal problems which can cause voice hoarseness. There may be reduced speech volume.
- Note any problem with language function (dysphasia). This is due to a lesion in the language areas of the dominant hemisphere.
Involuntary movements
Establish whether there is evidence of involuntary movements – for example, tremor, tics, chorea, hemiballismus, or orofacial dyskinesias.
History
Specific emphasis should be placed on the following:
Presenting complaint / Ask about the symptoms
- What are they?
- Which part of the body do they affect? Are they localized or more widespread?
- When did they start?
- How long do they last?
- Were they sudden, rapid or gradual in onset? Is there a history of trauma?
- Are the symptoms static or deteriorating, or are there exacerbations and remissions? For example, worsening of symptoms with hot environments – eg, sauna, hot bath or hot weather in demyelinating disorders (called Uhthoff’s sign).
- Does anything trigger the symptoms – eg, exercise, sleep, posture, or external stimuli such as light or smell?
Ask about any associated symptoms (other features of neurological disease):
- A headache.
- Numbness, pins and needles, cold or warmth.
- Weakness, unsteadiness, stiffness, or clumsiness.
- Nausea or vomiting.
- Visual disturbance.
- Altered consciousness.
- Psychological changes – eg, agitation, tearfulness, depression or elation, sleep disturbance.
- For children, ask about performance at school.
Past medical history
Some neurological problems can present years after a causative event.
- Enquire about other medical problems, past and present. These may give clues to the diagnosis. For example:
- A person in atrial fibrillation may be producing multiple tiny emboli.
- There may be vascular problems or recurrent miscarriages to suggest antiphospholipid syndrome.
- There may be diabetes mellitus.
- Ask about pregnancy, delivery, and neonatal health.
- Ask about any infections, convulsions, or injuries in infancy, childhood, or adult life. Particularly ask about the head or spinal injury, meningitis, or encephalitis.
Systematic inquiry
Systematic inquiry is very important here. For example:
- Loss of weight and appetite may suggest malignancy and this may be a paraneoplastic syndrome.
- The gain in weight may have precipitated diabetes mellitus.
- Polyuria may suggest diabetes mellitus. The difficulty with micturition or constipation may be part of the neurological problem but was not volunteered in the general history. In men, enquire about erectile dysfunction.
- Note smoking and drinking habits. Alcohol is a significant neurotoxin, both centrally and peripherally.
- Ask about drugs, including prescribed, over-the-counter, and illicit (such as cocaine usage that can be linked to cardiovascular problems). This includes complementary and alternative medicines.
- Ask about occupation and what it involves. There may be exposed to toxins. Is repetitive strain injury likely? Is there prolonged visual work that may predispose to a tension-type headache or a migraine? The job may involve driving but the patient has admitted to convulsions. He/she may work at heights or in a dangerous environment.
- Ask about marital status. Has there been recent bereavement or divorce which may have affected symptoms?
- Ask about sexual orientation and consider the likelihood of sexually transmitted infection – eg, syphilis, HIV.
Family history
Consider if there may be a genetic basis or predisposition. For example:
- A cousin with Duchenne muscular dystrophy or Becker’s muscular dystrophy would be very important for a boy who cannot run like his peers.
- Huntington’s chorea is unusual in that it is a familial disease that does not present until well into adult life.
- A family history of, for example, type 2 diabetes mellitus, cerebral aneurysm, neuropathies, epilepsy, migraine, or vascular disease may be important.
Examination
Examination of speech
- Look for spontaneous speech, fluency, and use of appropriate words during a conversation.
- Ask the patient to name objects.
- Ask the patient to carry out some commands to assess their comprehension.
- Ask the patient to read aloud. This can show evidence of any dyslexia.
- Ask the patient to repeat a simple sentence. Inability to do this suggests a conduction dysphasia.
- Look at the patient’s handwriting. There may be problems with the form, grammar or syntax, which may suggest a more global language problem and not just a speech disorder.
Examination of the neck
Examine the neck movements:
- Is there evidence of degenerative disease which may be producing radicular symptoms in the upper limbs? Examine flexion, extension, and rotation.
- Look for Lhermitte’s sign: neck flexion causes an electric shock-like feeling on the limbs. It is due to disease in cervical spinal cord sensory tracts (seen in, for example, multiple sclerosis, syringomyelia, tumors) .
- Is there any neck stiffness? This can be a sign of meningeal irritation. The chin can normally touch the chest when the neck is flexed but this is not possible if neck stiffness is present. This may be a sign of meningitis or subarachnoid hemorrhage.
- Palpate the supraclavicular fossae:
- Look for enlarged lymph nodes or cervical ribs.
Listen for any bruits:
- Listen at the carotid bifurcation at the angle of the jaw for carotid bruits.
- Listen over the supraclavicular fossa for vertebral or subclavian bruits.
- A common carotid bruit may be heard by listening between these two sites.
- Listen with the bell of the stethoscope over a closed eyelid for bruits due to cerebral arteriovenous malformations.
- Listen for cardiac murmurs to ensure that any bruit heard is not just due to the transmission of these.
- Note that just because a bruit is not heard, it does not mean that there is no significant stenosis present.
Cranial nerves
Examination of the cranial nerves takes practice. For their function and examination, see separate Examination of the Cranial Nerves article. This should include testing of the olfactory, optic, oculomotor, trochlear, abducent, trigeminal, facial, vestibulocochlear, glossopharyngeal, vagus, accessory and hypoglossal nerves.
Examination of the sensory system
See separate Neurological Examination of the Upper Limbs and Neurological Examination of the Lower Limbs articles. Both the upper and lower limbs should be examined. Work in a methodical way. A logical progression is required when examining each sensory modality. The following sensory modalities should be tested:
- Light touch and pinprick (sharp touch).
- Temperature.
- Proprioception (joint position sense).
- Vibration sense.
- Two-point discrimination.
Examination of the motor system
examined. The examination should include;
- Inspection.
- Tone.
- Power.
- Deep tendon reflexes.
- Superficial tendon reflexes.
- Co-ordination.
C1 to C5 Spinal Vertebra Information
- Most severe of the spinal cord injury levels.
- C2 to C3 – Usually fatal as a result of an inability to breathe.
- Requires 24 hour a day assistance.
- Paralysis in arms, hands, trunk, and legs.
- Will not be able to drive a car on their own.
- Ability to speak is sometimes impaired or reduced.
- If both arms and legs are affected, this is called tetraplegia or quadriplegia.
- May be able to use powered wheelchairs with special controls to move around on their own.
- The patient may not be able to breathe on his or her own, cough, or control bowel or bladder movements.
- Requires complete assistance with activities of daily living, such as eating, dressing, bathing, and getting in or out of bed.
C1 – Atlas – The Atlas is the topmost vertebra, and along with C2, forms the joint connecting the skull and spine. Its chief peculiarity is that it has nobody, and this is due to the fact that the body of the atlas has fused with that of the next vertebra.
C2 – Axis – Forms the pivot upon which C1 rotates. The most distinctive characteristic of this bone is the strong odontoid process (dens) which rises perpendicularly from the upper surface of the body. The body is deeper in front than behind and prolonged downward anteriorly so as to overlap the upper and front part of the third vertebra. Injuries to C-1 and C-2 can result in a loss of many involuntary functions including the ability to breathe, necessitating breathing aids such as ventilators or diaphragmatic pacemakers.
C3 – Injury to spinal bone three often causes pain, tingling, and sometimes numbness in the arms, neck, and head. If the fourth cervical vertebrae (C4) nerve root is also involved, pain is usually felt in the upper arms and shoulders, as well as the lower neck.
C4 – Cervical Vertebra – Quadriplegia and breathing difficulty – The fourth cervical (neck) vertebra from the top. Injuries above the C-4 level may require a ventilator for the person to breathe properly.
C5 – Quadriplegia with some shoulder and elbow function – 5th cervical vertebrae down from the base of the skull, found in the neck. C5 injuries often maintain shoulder and biceps control but have no control at the wrist or hand.
- C5 to C8 injuries – Corresponding nerves control the arms and hands, a person with this level of spinal injury may still be able to breathe on their own and speak normally.
C6 – Cervical Vertebra – Quadriplegia with shoulder, elbow, and some wrist function – The sixth cervical (neck) vertebra from the top. The next-to-last of the seven cervical vertebrae. An injury to the spinal cord between C6 and C7 vertebrae is called a C6-7 in
C7 – VertebraProminents – Quadriplegia with shoulder, elbow, wrist, and some hand function – The most distinctive characteristic of this vertebra is the existence of a long and prominent spinous process, hence the name vertebra prominent. In some subjects, the seventh cervical vertebra is associated with an abnormal pair of ribs, known as cervical ribs. These ribs are usually small, but may occasionally compress blood vessels (such as the subclavian artery) or nerves in the brachial plexus, causing unpleasant symptoms. C-7 and T-1 can straighten their arms but still may have dexterity problems with the hand and fingers. Injuries at the thoracic level and below result in paraplegia, with the hands not affected.C8 – Quadriplegia with normal arm function; hand weakness – Although there are seven cervical vertebrae (C1-C7), there are eight cervical nerves (C1-C8). All nerves except C8 emerge above their corresponding vertebrae, while the C8 nerve emerges below the C7 vertebra. In other words, C8 is a nerve root, not vertebrae.
Thoracic Vertebrae (T1 to T12)
The thoracic vertebrae increase in size from T1 through T12 and represent the 12 thoracic vertebrae. The thoracic vertebrae are situated between the cervical (neck) vertebrae and the lumbar vertebrae. These thoracic vertebrae provide attachment for the ribs and makeup part of the back of the thorax or chest. Damage or SCI’s above the T1 vertebra affects the arms and the legs. Injuries below the T1 vertebra affect the legs and trunk below the injury, but usually, do not affect the arms and hands. Paralysis of the legs is called paraplegia. Paralysis of the arms AND legs is called quadriplegia. The most common fractures of the spine occur in the thoracic (midback) and lumbar spine (lower back) or at the connection of the two (thoracolumbar junction). These fractures are typically caused by high-velocity accidents, such as a car crash, or a fall from height.
- T1 to T6 – Paraplegia with loss of function below mid-chest; full control of arms
- T1 to T8 – Most often control the hands, but poor trunk control as the result of lack of abdominal muscle control.
- T6 to T12 – Paraplegia with loss of function below the waist; good control of torso
- T9 to T12 – Allow good trunk control and abdominal muscle control. Lumbar and Sacral injuries yield decreasing control of the hip flexors and legs. Individuals with SCI also experience other changes. For example, they may experience dysfunction of the bowel and bladder.
- Corresponding nerves affect muscles, upper chest, mid-back and abdominal muscles.
T1 to T5 Thoracic Nerves
- Can learn to drive a modified car.
- Arm and hand function is usually fairly normal.
- Will most likely need to use a manual wheelchair.
- Injuries usually affect the trunk and legs (paraplegia).
T1 – Comparatively speaking, T1 is the smallest of all thoracic vertebrae. The T1 vertebra is the first (uppermost) of the twelve (12) thoracic vertebrae that make up the central and largest section of the spinal column between the lumbar vertebrae below and the cervical vertebrae above.
T2 – The second vertebra in the thoracic spine is responsible for helping to support the rib cage. The T2 vertebra possesses facets that create joints with two of the ribs, thus helping to keep the thoracic spine far more stable than the cervical spine in the neck or the lumbar spine in the lower back.
T2 vertebra degeneration includes – Herniated, bulging or prolapsed discs, Bone spurs, Facet disease, Forms of osteoarthritis and Traumatic or sports-related injuries.
T3 – The third thoracic vertebrae is a small vertebra in the upper middle back that plays an integral role in supporting the rib cage. The anterior aspect of the upper thoracic spine is a difficult region to approach in spinal surgery.
T4 – Spinal cord transection at T4 results in severe damage of the nervous tissue, with impairment of motor, sensory and autonomic functions.
T4 syndrome is a relatively uncommon condition in which spinal injury at the T4 vertebra causes a set of symptoms including diffuse arm pain and pins and needles or numbness in the upper arm.
T5 – The T5 vertebra, as well as the rest of the thoracic spine, provides a stable foundation for the human rib cage.
T6 – An injury at the level of the T6 (thoracic) spinal cord results in damage to the autonomic nervous system, both the sympathetic and parasympathetic divisions, affecting the function of major abdominal organs.
T7 – The T7 vertebra is in the middle of the twelve (12) thoracic vertebrae of the torso and the center of the spinal column. Thoracic vertebrae play an important role, not only in the protection of the spinal cord but also in the protection of vital organs. A vertebral compression fracture refers to a break of the vertebral body, most often below the T7 level of the thoracic spine (upper back), and is most commonly caused by weakened bone resulting from osteoporosis. Most vertebral compression fractures result in a loss of more than 15% to 20% of the height of the vertebra
T8 – T8 vertebra is toward the lower (caudal) end of the twelve (12) thoracic vertebrae within the central, torso section of the spine. Like other spinal vertebrae, the T8 primarily protects and encases the spinal cord. The T8 is also at the same level as the xiphoid process. The eighth thoracic spinal nerve runs beneath the T8. Throughout the thoracic spine, discs like those above and beneath the T8 vertebra can become damaged and cause painful symptoms.
T9 – T9 to T12 are known as transition vertebrae. The lumbar cord is situated between T9 and T11 vertebrae. T9 to T12 injuries can be classified as either complete or incomplete injuries. Complete injuries result in the total loss of movement and sensation below the point of injury, while incomplete injuries indicate that some function below the level of injury is retained.
T10 – T10 is situated at the umbilicus. The T10 vertebra is near to the bottom of the twelve (12) thoracic vertebrae (T1-T12) within the torso and makes up the central portion of the spinal column. This particular vertebra has a complete articular facet and the thoracic spinal nerves pass out under it. T10 innervates the muscles of the lower abdomen. It is part of the section of the spinal cord which is most vulnerable to injury due to the area’s high level of flexibility. An injury in this area will most likely experience a limited or complete loss of use of the muscles in the lower abdomen, buttocks, legs, and feet. The extent of disability is determined by damage done to the T10 vertebra. Partial damage may cause weakness, numbness, lack of muscle control, or loss of the use of one side of the lower body. Complete damage could result in the loss of use of the lower body (paraplegia).
T11 – The ribs connected to T11 and T12 at the bottom of the thoracic spine do not attach the sternum in front, but do provide protection for the kidneys in the back of the body. Because these levels have slightly less stability, they are slightly more prone to problems that can cause pain. A person with a T11 vertebral injury may have or recover sensations in the L1 through L4 dermatomes which include the front of the leg down to the mid-shin level. In addition, such a patient should recover hip extensors, knee extensors, and even ankle dorsiflexion. However, the sacral functions, including bowel and bladder and many of the flexor functions of the leg may be absent or weak.
T12 – T12 ends just above the hip girdle. T12 bears the most weight of any thoracic vertebra, making it the strongest thoracic vertebra, but also the most susceptible to stress-related injuries. Compression fractures of the spine usually occur at the bottom part of the thoracic spine (T11 and T12) and the first vertebra of the lumbar spine (L1). The most common thoracic spinal cord injury involves T11 and T12.
Lumbar Vertebrae (L1 to L5)Lumbar nerves (L1 to L5) injuries generally result in some loss of function in the hips and legs. Often there is little or no voluntary control of bowel or bladder, but patients usually manage on their own with the use of special equipment. Depending on strength in the legs, some patients may need a wheelchair and may also walk with braces. The lumbar vertebrae graduate in size from L1 through L5. These vertebrae bear much of the body’s weight and related biomechanical stress. The lumbar vertebrae are also the largest segments of the movable part of the vertebral column and are characterized by the absence of the foramen transversarium within the transverse process, and by the absence of facets on the sides of the body. Some individuals have four lumbar vertebrae, while others have six. Lumbar disorders that normally affect L5 will affect L4 or L6 in these individuals.
L1 – The first lumbar vertebra is at the same level as the ninth rib. This level is also called the important transpyloric plane since the pylorus of the stomach is at this level.
L2 – Injuries to the spinal column at L2 or lower will damage the tip of the spinal cord, called the CONUS, or the spray of spinal roots that are descending to the appropriate spinal vertebral levels to exit the spinal canal or the caudal equine.
L3 – The L3 vertebra is in the middle of the five lumbar vertebrae in the lower back portion of the spinal column. The L3 vertebra, or third lumbar vertebra, is one of the most common sites for the occurrence of a herniated disc and other spinal conditions that can cause chronic lower back pain. A lot of motion in the back is divided between these five motion segments with segments L3 – L4 and L4 – L5 taking most of the stress. L3 – L4 and L4 – L5 segments are most likely to break down from wear and tear causing such conditions as osteoarthritis. L2 and L3 cover the front part of the thighs.
L4 – The most likely to herniate (herniated disc, bulging disk, compressed disk, herniated intervertebral disk, herniated nucleus pulposus, prolapsed disk, ruptured disk, slipped disk). The effects of this can cause pain and numbness that can radiate through the leg and extend down to the feet (sciatica). Spondylolysis and spondylolisthesis are conditions that affect the moveable joints of the spine that help keep the vertebrae aligned one on top of the other. Spondylolysis is actually a weakness or stress fracture in one of the bony bridges that connect the upper and lower facet joints. This fracture can happen at any level of the spine but usually occurs at the fourth (L4) or fifth (L5) lumbar vertebra. L4 and L5 fractures are commonly the results of a high impact trauma from falls or m
The sacrum is shaped differently in males and females. In females,s the sacrum is shorter and wider than in males. The Sacrum is located behind the pelvis. Five bones (abbreviated S1 through S5) fused into a triangular shape, from the sacrum. The sacrum fits between the two hipbones connecting the spine to the pelvis located just below the lumbar vertebrae. The Sacrum consists of four or five sacral vertebrae in a child, which become fused into a single bone after age 26. The sacrum forms the back wall of the pelvic girdle and moves with it.
The first three vertebrae in the sacral have transverse processes which come together to form wide lateral wings called alae. These alae articulate with the blades of the pelvis (ilium).
As part of the pelvic girdle, the sacrum forms the back wall of the pelvis and also forms joints at the hip bone called the sacroiliac joints. The sacrum contains a series of four openings on each side through which the sacral nerves and blood vessels run. The sacral canal runs down the center of the sacrum and represents the end of the vertebral canal.
Back pain or leg pain (sciatica) can typically arise due to injury where the lumbar spine and sacral region connect (at L5 – S1) because this section of the spine is subjected to a large amount of stress and twisting.
People with rheumatoid arthritis or osteoporosis are inclined to develop stress fractures and fatigue fractures in the sacrum.
The bottom of the spinal column is called the coccyx or tailbone. It consists of 3 to 5 bones that are fused together in an adult. Many muscles connect to the coccyx.
Sacral Nerves (S1 to S5) injuries generally result in some loss of function in the hips and legs. Little or no voluntary control of bowel or bladder, but can manage on their own with special equipment Most likely will be able to walk.
S1 –
- L5 to S1 Isthmic Spondylolisthesis: A small fracture in the facet joints can allow the L5 vertebra to slip forward over the S1 vertebra, impinging the nerve root and leading to leg pain and other symptoms.
- L5-S1 disc herniation: Occurs when the inner portion leaks out and touches the nearby nerve root, causing pain to radiate in the lower back and/or down the leg.
- L5-S1 degenerative disc disease: If the L5-S1 disc is compromised, the L5-S1 disc itself can become a source of lower back and/or leg pain.
S2 – S2 is located at the level of the posterior superior iliac spine.
S2- Covers the back of the thighs.
S3 – S3 cover the medial side of the buttocks.
S4 – S4-5 covers the perineal region.
S5 – S5 is the lowest dermatome and represents the skin immediately at and adjacent to the anus.
Sacral Nerves (S1 to S5) injuries generally result in some loss of function in the hips and legs. Little or no voluntary control of bowel or bladder, but can manage on their own with special equipment Most likely will be able to walk
S2 – S2 is located at the level of the posterior superior iliac spine. S2 covers the back of the thighs.
S3 – S3 cover the medial side of the buttocks.
S4 – S4-5 covers the perineal region.
S5 – S5 is the lowest dermatome and represents the skin immediately at and adjacent to the anus.
Treatment Spinal Cord Injury
First Aid
Never move anyone who you think may have a spinal injury unless it is absolutely necessary. For example, if you need to get the person out of a burning car, or help them to breathe.
Keep the person completely still and safe until medical help arrives.
- Call the local emergency number, such as 911.
- Hold the person’s head and neck in the position in which they were found. Do not try to straighten the neck. Do not allow the neck to bend or twist.
- Do not allow the person to get up and walk unassisted.
If the person is not alert or responding to you:
- Check the person’s breathing and circulation.
- If needed, do CPR. Do not do rescue breathing, do chest compressions only.
Do not roll the person over unless the person is vomiting or choking on blood, or you need to check for breathing. If you need to roll the person over:
- Have someone assist you.
- One person should be located at the person’s head; the other at the person’s side.
- Keep the person’s head, neck, and back in line while you roll him or her onto one side.
Do Not
- Do not bend, twist, or lift the person’s head or body.
- Do not attempt to move the person before medical help arrives unless it is absolutely necessary.
- Do not remove a football helmet or pads if a spinal injury is suspected.
Non-surgical
- Rest – It is important that the patient take proper rest and sleep and avoid any activities which will further aggravate the disc bulge and its symptoms. Many minor disc bulges can heal on their own with rest and other conservative treatments.
- Cervical Pillow – It is important to use the right pillow to give your neck the right type of support for healing from a cervical disc bulge and also to improve the quality of sleep.

Specific treatment for lumbar disk disease will be determined by your health care provider based on
- Your age, overall health, and medical history
- Extent of the condition
- Type of condition
- Your tolerance for specific medications, procedures, or therapies
- Expectations for the course of the condition
- Your opinion or preference
Typically, conservative therapy is the first line of treatment to manage lumbar disk disease. Approach for Treating and Reversing a Disc Bulge about half of the disc bulges heal within six months and only about 10% of the disc bulges require surgery. So, the good news is that conservative treatment for a disc bulge helps in treating as well as reversing the disc bulges.
- Ice & Moist Heat Application

Ice application where the ice is wrapped in a towel or an ice pack for about 20 minutes to the affected region, thrice a day, helps in relieving the symptoms of a disc bulge. Heat application in the later stages of treatment also provide the same benefit.
- Hot Bath
Taking a hot bath or shower also helps in dulling the pain from a disc bulge. Epsom salts or essential oils can be added to a hot bath. They will help in soothing the inflamed region.
- Traction

- Massage therapy – may give short-term pain relief, but not a functional improvement, for those with acute lower back pain. It may also give short-term pain relief and functional improvement for those with long-term (chronic) and sub-acute lower pack pain, but this benefit does not appear to be sustained after 6 months of treatment. There does not appear to be any serious adverse effects associated with massage.
- Acupuncture – may provide some relief for back pain. However, further research with stronger evidence needs to be done.
- Spinal manipulation – is a widely-used method of treating back pain, although there is no evidence of long-term benefits.
- “Back school” – is an intervention that consists of both education and physical exercises. A 2016 Cochrane review found the evidence concerning back school to be very low quality and was not able to make generalizations as to whether the back school is effective or not.
- Patient education on proper body mechanics (to help decrease the chance of worsening pain or damage to the disk)
- Physical therapy – which may include ultrasound, massage, conditioning, and exercise
- Weight control
- Use of a lumbosacral back support
Medications for Spinal Cord Injury
- Analgesics – Prescription-strength drugs that relieve pain but not inflammation.
- Antidepressants: Drugs that block pain messages from your brain and boost the effects of endorphins (your body’s natural painkillers).
- Medication – Common pain remedies such as aspirin, acetaminophen, ibuprofen, and naproxen can offer short-term relief. All are available in low doses without a prescription. Other medications, including muscle relaxants and anti-seizure medications, treat aspects of spinal stenoses, such as muscle spasms and damaged nerves.
- Corticosteroid injections – Your doctor will inject a steroid such as prednisone into your back or neck. Steroids make the inflammation go down. However, because of side effects, they are used sparingly.
- Anesthetics – Used with precision, an injection of a “nerve block” can stop the pain for a time.
- Muscle Relaxants – These medications provide relief from spinal muscle spasms.
- Skeletal muscle relaxers – may also be used. Their short-term use has been shown to be effective in the relief of acute back pain. However, the evidence of this effect has been disputed, and these medications do have negative side effects.
- Neuropathic Agents: Drugs(pregabalin & gabapentin) that address neuropathic—or nerve-related—pain. This includes burning, numbness, and tingling.
- Antibiotic – to the management of bowel & bladders control and protect against further infection. Infection causes should be treated with appropriate antibiotic therapy
- Topical Medications – These prescription-strength creams, gels, ointments, patches, and sprays help relieve pain and inflammation through the skin.
- Calcium & vitamin D3 – to improve bones health and heal fractures.
- Glucosamine & diecarin – can be used to tighten the loose tension and regenerate cartilage or inhabit the further degeneration of cartilage.
- Corticosteroid – to heal the nerve inflammation and clotted blood in the joints.
- Dietary supplement -to remove the general weakness & improved the health.
- Lesion debulking – is required for space-occupying lesions – eg, tumors, abscesses.
- If surgery cannot be performed – radiotherapy may relieve cord compression caused by malignant disease.
- Radiation therapy and chemotherapy – may have a role in treatment if the cauda equina syndrome is caused by the tumor.
- Support or brace – A pelvic belt can be used to stabilize a joint that is too loose until the inflammation and pain subside.
- Joint injections – Numbing injections into the sacroiliac joint are used diagnostically to help identify the cause of the but are also useful in providing immediate pain relief. Typically, an anesthetic is injected along with anti-inflammatory medication.
Other treatment options
- Other treatment options – may be useful in certain patients, depending on the underlying cause of the CES
- Anti-inflammatory agents, including steroids, can be effective in patients with inflammatory causes – eg, ankylosing spondylitis.
- Patients with spinal neoplasms should be evaluated for chemotherapy and radiation therapy.
- Weakness – Physiotherapy may be helpful if there is no inflammatory component such as that found in arachnoiditis where exercise might exacerbate the condition and cause flare-ups.
- Sensory Loss – Little conventional treatment exists for sensory loss in cauda Equina syndrome, although in conditions such as Multiple Sclerosis use of vitamin B complex is considered to have potentially beneficial effects.
- Sore Feet – Loss of muscle tone and control over the movement of the foot may lead to foot pain. If foot drop is a notable issue, a brace to hold it in position may help. It is important; however, to attempt to maintain as much muscle tone as possible as well as a range of movement (ROM). Exercises might help.
- Sexual Dysfunction – Sexual dysfunction is very hard for people to talk about at times. It might be best to pursue advice from specialists. If no physical treatment is feasible for improving function, the person and their sexual partner might pursue counseling which might help to lessen the impact of this disability on not only the person affected but their partner.
- Depression – Depression is an understandable reaction to a form of debilitating illness. Antidepressant medication should be reserved for severe depression. Counseling and support are the preferred methods of managing depression. Sharing experiences may help people with cauda Equina syndrome to come to terms with the disabilities associated with cauda Equina syndrome.
- Poor Circulation – Poor circulation is a common issue in cauda Equina syndrome. The person’s feet may be cold and turn white, then red when re-warmed (also known as, ‘Raynaud’s syndrome,) as well as chilblains. Some medications exist that can be taken, yet it is most likely best to use general measures such as avoiding getting cold feet and foot massage with warm oil to help improve the person’s circulation. Avoid extremely hot baths after the feet have been cold because it will most likely cause chilblains.
- Postoperative care – includes addressing lifestyle issues (eg, obesity), and also physiotherapy and occupational therapy, depending on residual lower limb dysfunction.
- Prolotherapy – the practice of injecting solutions into joints (or other areas) to cause inflammation and thereby stimulate the body’s healing response – has not been found to be effective by itself, although it may be helpful when added to another therapy.
- Herbal medicines – as a whole, are poorly supported by evidence. The herbal treatments Devil’s claw and white willow may reduce the number of individuals reporting high levels of pain; however, for those taking pain relievers, this difference is not significant. Capsicum, in the form of either a gel or a plaster cast, has been found to reduce pain and increase function.
- Behavioral therapy – may be useful for chronic pain. There are several types available, including operant conditioning, which uses reinforcement to reduce undesirable behaviors and increase desirable behaviors;
- Cognitive-behavioral therapy – which helps people identify and correct negative thinking and behavior; and respondent conditioning, which can modify an individual’s physiological response to pain. Medical providers may develop an integrated program of behavioral therapies. The evidence is inconclusive as to whether mindfulness-based stress reduction reduces chronic back pain intensity or associated disability, although it suggests that it may be useful in improving the acceptance of existing pain.
- Tentative evidence supports neuroreflexotherapy (NRT) – in which small pieces of metal are placed just under the skin of the ear and back, for non-specific low back pain
Rehabilitations
Physiotherapy
Every individual with Spinal cord injury presents with different symptoms and needs, depending on the level and extent of the damage to the spinal cord. Each individual will be assessed by their therapist and have treatment tailored to their needs and goals. Some of the physiotherapy treatments we offer can help to:
- Increase muscle strength through strengthening and mobilization exercises
- Improve balance and mobility through assessment of different seating and mobility aids and postural re-education
- Increasing sensation through sensory stimulation
- Reduce muscle stiffness, spasms, and pain through stretching programs
- Reduce the risk of falls through balance work, gait re-education, and training
- Treatment and management of the chest and respiratory system through advice, education on the management of infections, and exercises to improve breathing
- Increase independence and quality of life through management of positioning in bed and seating
- Master the techniques for transfers from basic through to advanced levels
- Practice and problem solve wheelchair skills in real home environment settings
- Offer individual SCI education
- Access Functional Electrical Stimulation (FES) and identify which modalities are appropriate
- Trial and assess the benefits of the Exoskeleton as an adjunct to the rehabilitation
- Work on gait training including access to the LiteGait partial weight-bearing device
Occupational Therapy
Occupational therapy is a crucial process in rehabilitation since it eases societal role finding [rx]. It focuses on enhancing daily life activity execution and fine movement, by searching for total independence or performing compensatory strategies to adapt [rx, rx, rx] as well as patient’s environment adaption (home, transportation, or workplace) to achieve total inclusion with its remaining abilities.
It demands equipment and techniques for transferring from one surface to another, dressing, bathing, grooming, feeding, cooking, respiratory exercises, and vesical and intestinal control. Besides, it also trains on wheelchair use and provides counseling for house modifications like ramp addition, bath chair incorporation, and current insulation [rx, rx].
Our specialist OTs aim to improve areas of personal care, work or leisure that are becoming difficult. This can be achieved through:
- Functional activities independently or in groups
- Assessing function in a home environment and establishing any needs for equipment, adaptations, or further rehabilitation
- Community skills: working on managing in the community (wheelchair skills etc.) via trips to the shops/pub/friend’s house
- Hand therapy including splinting and exercise programs
- Assessment of wheelchair set-up
- Advice and management of pressure relief through bed positioning and seating adaptations
- Management and education to help you to adapt and manage altered sensation
- Vocational rehabilitation
- Exploration of past and new hobbies & leisure activities in your wheelchair
Orthotics
For people with spinal cord injury our specialist orthodontist, working with the team, can help by designing and fitting orthoses to best complement your treatment and rehabilitation. These include:
- Orthotics to prevent foot drop and aid walking
- Night and day resting splints to maintain alignment and prevent contractures
- Insoles to improve alignment, proprioception, and gait
- Alteration to shoes to assist with leg length discrepancies, alignment and improve mobility
- Custom made spinal supports
Neuropsychology
Following a traumatic injury or disease, people often find it difficult to cope with the sudden changes to their mobility, social life, and overall lifestyle. Our clinical neuropsychologists can help to provide:
- Detailed assessment of a clients’ functioning in particular their cognition, behavior, and emotional state
- Providing advice, consultation, teaching, and supervision to other professionals as well as family and carers
- Management and advice for anxiety and changes in mood
Speech and Language Therapy
Difficulties in speech and swallowing are not often experienced in incomplete spinal cord injuries, but this can depend on the level of injury. Difficulties in written and non-verbal communication can often be experienced. Our specialist speech and language therapists can assist with:
- Advice and treatment with writing tools and communication aids
- Treatment at the center or in your own home
- Assistance with written communication including adaptive equipment
Range of movement, strength, and stretching exercises – Range of movement refers to the normal movement of a joint; hence range of movement exercises are those that promote joint mobility and flexibility.
Studies have observed that these exercises improve function for daily life activities [rx], prevent contractures, protect tenodesis effect [rx], strengthen paralyzed muscles, promote nerve and cerebral remodeling, and improve spinal microenvironment and functional prognosis [20]. For the protection of the joint structure and preservation of muscle tone, sandbags, pillows, or orthotics are usually used. Exercise is important for strengthening the muscles of the upper limbs, emphasizing the rotation of the shoulders for the use of crutches or wheelchairs. These exercises will help in the mobilization and independence in daily life activities. In patients with incomplete SCI, walking potential is high, so sitting, parallel bars and balance exercises should be done [rx].
Muscle maintenance and strengthening — Spinal cord injury recovery and rehabilitation means maintaining and strengthening your muscles. Our physical therapists will guide you through an individualized treatment plan to maximize your improvement in strength, coordination, and endurance.
Functional electrical stimulation – Functional electrical stimulation is a technique that artificially activates sensory-motor systems through electrical current pulses, producing action potentials in afferent and efferent neural pathways to stimulate muscles and generate movement [rx]. This procedure is added to other therapies to increase mobility, sensory feedback, and muscle activity to decrease atrophy. It also provides cardiorespiratory fitness; improves posture and trunk stability [rx]; prevents contractures, pressure ulcers, and orthostatic hypotension [23]; promotes nerve restoration, and prevents peripheral nerve deterioration [rx].
Functional electrical stimulation is a technique that artificially activates sensory-motor systems through electrical current pulses, producing action potentials in afferent and efferent neural pathways to stimulate muscles and generate movement [rx]. The main elements of a FES system are the battery, an electronic stimulator, control unit, wiring, and electrodes. The controller can work through a switch, joystick, or voice. There are different types of electrodes, superficial, intramuscular percutaneous, implantable, and epimysial; however the commercially available are the superficial ones, which should be placed over the skin above the nerves to be stimulated; the rest of the electrodes are for research purposes only. The electrodes must be of low impedance, flexible, and easy to don and doff [rx]. The electrical parameters of these systems are waveforms, amplitude, pulse width, reciprocity, ramp, and duration; all of these are combined to generate an electrical current and must be adjusted to achieve the desired response [rx, rx].
Epidural electrical stimulation of the spinal cord – This strategy requires a device to be implanted through a laminectomy over the dura mater of the spinal cord [rx]. The device delivers a rhythmical afferent electrical current to posterior nerve roots to activate central circuits that regulate movement, pain, and the cardiorespiratory system [rx].
It is believed that EES activates two pathways: The first one stimulates afferent dorsal pathways that synapse with motor neurons; the second pathway directly stimulates motor neurons through stimulation of efferent motor nerves [rx].
Studies in SCI patients have shown that this strategy decreases fatigue [rx], improves cardiovascular and respiratory fitness, increases lean body mass, and improves bladder voiding [rx]. The main disadvantage of EES is that it requires surgery for device insertion, which implicates the risk of infection, hematoma, or injury because of the device [rx].
This experimental strategy requires a device to be implanted through a laminectomy over the dura mater of the spinal cord [rx]. The device delivers a rhythmical afferent electrical current to posterior nerve roots to activate central circuits that regulate movement, pain, and the cardiorespiratory system [rx].
It is believed that EES activates two pathways: The first one stimulates afferent dorsal pathways that synapse with motor neurons; the second pathway directly stimulates motor neurons through stimulation of efferent motor nerves [rx].
Studies in SCI patients have shown that this strategy decreases fatigue [rx], improves cardiovascular and respiratory fitness, increases lean body mass, and improves bladder voiding [rx]. The main disadvantages of EES are that it requires surgery for device insertion, which implicates the risk of infection, hematoma, or injury because of the device [rx], it is expensive, and it does not yet establish a standard number of sessions and parameter configurations since multiple studies have shown that outcomes vary in each patient due to SCI heterogeneity [rx].
It is worth mentioning that this technique is used merely for research purposes only and it is not approved by health authorities. The evidence that exists to date is not enough to justify its use, since it has been studied only in specific small cohorts of patients or single patients with SCI and there are no clinical trials with this method [rx, rx].
Transcutaneous electrical nerve stimulation (TENS) – TENS is a high- and low-frequency electrical current therapy. It is used for pain management, but many other benefits have been observed, such as balance and proprioception improvement and spasticity decrease [rx]. To date, its mechanism of action is unknown; however, different theories assume it works by modulating inhibitory spinal circuits, by activating afferent neurons, or by inducing central nervous system plasticity [rx]. When applying it, it is necessary to consider electrode positioning, frequency, and pulse intensity; though, there is not a consensus on how long sessions should last and how much frequency has to be applied. The main advantages of this therapy are that it is low cost, it is easy to apply since the patient can do it by himself/herself, and there are no side effects reported yet [rx, rx].
Dry needling – Dry needling is an invasive procedure that consists of reaching muscle myofascial trigger points (MTPs) with a needle [rx]. MTPs are small, tense muscle nodules that cause pain, cause weakness, and limited range of motion [39].
It is considered that dry needling stimulation inhibits spontaneous electrical activity in MTPs by diminishing the availability of acetylcholine in the motor endplate (it is believed that MTP originates here); consequently, muscle fiber relaxes, promoting pain and spasticity reduction and improving gait speed and stability in patients with incomplete injury [rx, rx]. It is worth mentioning that more studies have to be made to set the frequency, duration, and intensity of sessions to obtain desirable outcomes [rx].
Exoskeletons – Exoskeletons are battery-powered robotic devices that adjust to the patients’ limbs; they can be operated with manual or oral control or a micromovement detector to ease mobility and gait [rx, rx].
Two main objectives of exoskeletons are promoting recovery through repeated movements to increase neural plasticity and assist mobility [rx]. ReWalk™ and Indego™ are two community use exoskeletons [rx] that enable walking, sitting, and climbing stairs up and down [rx, rx]. Their use has shown improvements in quality of life, body composition, bone density, neuropathic pain, and spasticity [42] and an increase in gait speed [rx], a number of steps, and distance tests before and after 90 days of training [rx].
Redeveloping motor skills – Physical, occupational, and speech therapists will help you optimize your ability to accomplish daily living activities with your current level of function while helping you progress towards greater skill and independence.
Indoor and outdoor Activities – Our rehabilitation facility was designed with both indoor and outdoor spaces including an indoor/outdoor gym experience and rehabilitation courtyard, which will offer important therapeutic challenges during your rehabilitation stay.
Seating and mobility clinic – When a manual or power wheelchair is required, our dedicated team of seating and positioning experts is essential for providing the best wheelchair equipment and accessories possible. Our clinic will also act as a partner in finding the right piece of adaptive sports or adventure gear to keep you active and healthy.
Mobility garage – We offer space to bring your vehicle into a climate-controlled environment. At our mobility garage, you can practice entering and exiting your vehicle and explore adaptive equipment that will help you return to driving sooner. This space will also serve as a showcase for the latest accessible vehicles and mobility technology.
Driving evaluation – An advanced driving simulator for hospital and community patients is available for practicing driving skills before returning to the road. An occupational therapy driving instructor will help assess your vision, reaction time, and cognitive processing speed to accurately determine your readiness to drive. Once we complete these tasks, the therapist will accompany you in a car on the road and monitor your progress.
Education and training – A rehab education specialist provides a comprehensive education program for patients, families, and caregivers during your hospital stay. Outpatient education forums occur throughout the year to bring you the latest information about spinal cord injury research and community resources. Busy family members and care providers can participate remotely using computers and video conferencing.
Prosthetics and orthotics fitting and training – We utilize orthotics and prosthetics to help assist you with your mobility and daily activities. New 3D printing technology allows us to quickly create custom solutions for your particular needs.
Hybrid Program – At Brooks Rehabilitation, we recognize that neuro-recovery takes a lot of time and hard work. Our goal is to provide therapy in the inpatient rehabilitation setting that can be continued as patients or their family members progress. To support this, our Hybrid Program is designed to bridge the gap from inpatient rehabilitation to outpatient by offering structured exercise-based programs. Our Hybrid program utilizes a variety of technologies including functional electrical stimulation, virtual reality, and computer/tablet applications and games to maximize your or your family member’s recovery. We utilize an ergonomic exoskeleton with integrated springs and computer-based games to simulate functional activities in a 3D workspace. Ultimately, the hybrid program allows patients with a variety of spinal cord injury symptoms to supplement their structured, scheduled therapy with additional exercises to further their rehabilitation.
FES Bike – Functional electrical stimulation of the peripheral nerves along with the patterned movement of the bike allows the muscles to work even if a patient has limited or no muscle control due to their spinal cord injury.
Bodyweight support – Utilizes a body harness that is worn by the patient and suspended from the ceiling and/or bodyweight support device. Bodyweight support allows for a percentage of a patient’s weight to be offloaded by the device in order to create a permissive environment for challenging activities such as walking, jumping, and squatting.
Circuit Training – A combination of strength, balance, and endurance activities that are individually prescribed to promote neurorecovery after a spinal cord injury.
References







{kind=link}
{kind=link}
{kind=link}
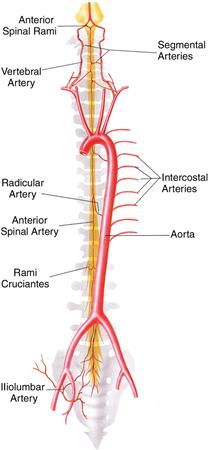{kind=link}
{kind=link}